Cricothyroidotomy, also known as cricothyrotomy refers to the creation of a communication between airway and skin via the cricothyroid membrane. It may be achieved by needle cricothyrotomy or by open or percutaneous cricothyroidotomy technique. Advantages of cricothyroidotomy compared to tracheostomy include simplicity, speed, relatively bloodless field, minimal training required, and avoiding hyperextending the neck in patients with possible cervical spinal injury.
Indications
Airway obstruction proximal to the subglottis
Respiratory failure
Pulmonary toilette in patients unable to clear copious secretions
Bronchosopy
For indications (1) and (2), cricothyroidotomy is generally done as an emergency temporising procedure when a patient cannot be intubated, or when tracheostomy would be too time consuming or difficult. Following cricothyroidotomy the patient should be intubated or a formal tracheostomy done within 24hrs to avoid complications such as glottic and subglottic stenosis.
Contraindications
Inability to identify surface landmarks (thyroid cartilage, cricoid, cricothyroid membrane) due to e.g. obesity, cervical trauma
Airway obstruction distal to subglottis e.g. tracheal stenosis or transection
Laryngeal cancer: Other than for an extreme airway emergency, avoid a cricothyroidotomy so as not to seed the soft tissue of the neck with cancer cells
Coagulopathy (other than emergency situation)
Cricothyroidotomy in children
The cutoff age beyond which surgical cricothyroidotomy can be safely performed is unclear. The most conservative cutoff age quoted is 12yrs; in young children the cricothyroid membrane is smaller, the larynx is more funnel-shaped, rostral, and compliant and cricothyroidotomy may be more prone to causing subglottic stenosis. Hence needle cricothyrotomy (12–14 gauge cannula passed over a needle) is preferred.
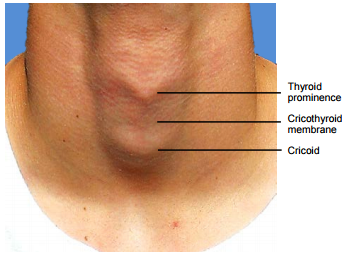
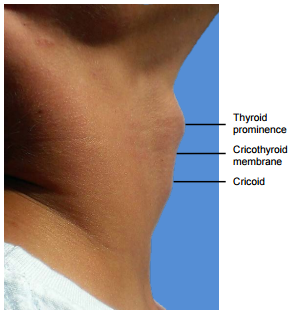
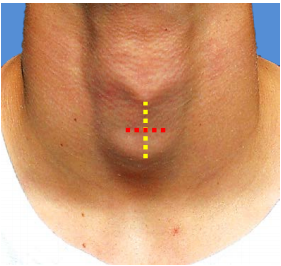
Surface anatomy (Figures 1a, b)
With the neck in a neutral or extended position, identify the midline thyroid prominence or “Adam’s apple”. Moving inferiorly, the next solid prominence in the midline is the cricoid cartilage. Immediately above the cricoid the finger slips into the depression of the cricothyroid membrane.
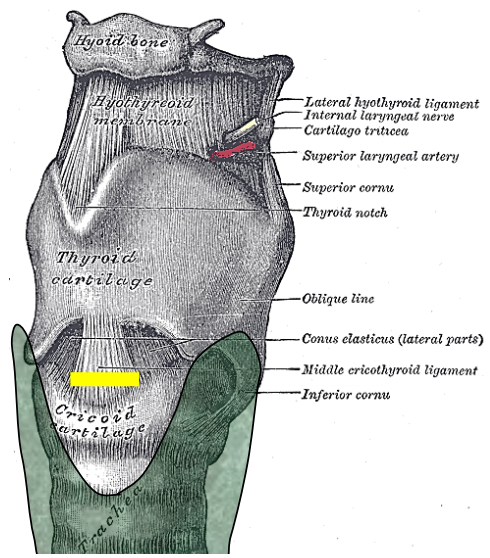
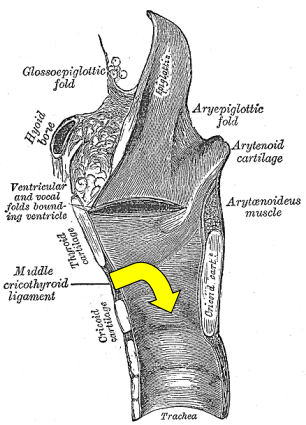
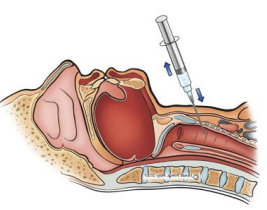
A cricothyroidotomy enters the larynx in the midline just below the vocal cords. The incision passes through skin, subcutanous fat, middle cricothyroid ligament of cricothyroid membrane, and mucosa of subglottic larynx (Figure 2).
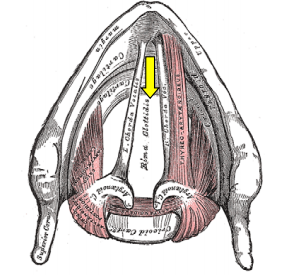
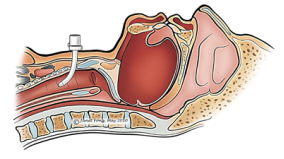
Figure 2: Relations of thyroid cartilage, cricothyroid membrane, cricoid cartilage, and thyroid gland (Brown) to location of cricothyroidotomy (Yellow line)Figure 3: Note proximity of tube to vocal cords, and relationship to cricoid ring
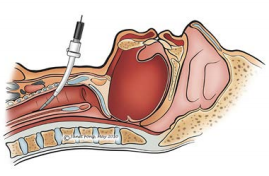
The tube then passes through the cricoid ring, which is the narrowest part of the upper airway (Figure 3, 4).
Figure 4: Note proximity of tube to vocal cords, and relationship to cricoid ring
The thyroid isthmus typically crosses the 2nd and 3rd tracheal rings, and is out of harm’s way, unless a pyramidal thyroid lobe is present (Figure 2). The only blood vessels that may be encountered are the anterior jugular veins (off the midline), and the cricothyroid arteries.
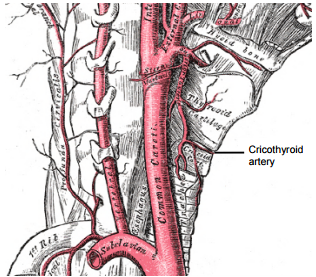
The cricothyroid artery is a small branch of the superior thyroid artery and courses across the upper part of the cricothyroid membrane and communicates with the artery of the opposite side (Figure 5). Therefore incise the membrane along the superior margin of the cricoid.
Figure 5: Cricothyroid artery
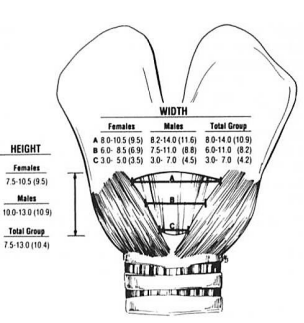
The dimensions of the cricothyroid membrane have a bearing on the size of endotracheal or tracheostomy tube to be used; the outer diameter (OD) of the tube should not exceed the diameter of the cricothyroid opening so as to avoid injury to the larynx. Even though the cricothyroid membrane measures 30mm in the horizontal plane, the gap between the cricothyroid muscles through which the tube has to pass is much less (Figure 6). Based on studies of the dimensions of cricothyroid membranes 1,2,3 it has been recommended that a tube of no more than 9-10mm OD be used 1; This corresponds to a 7mm ID tube. An alternative suggestion is to select a tube which is 1mm smaller than would normally be used for oro-tracheal intubation. 2 If a Shiley tracheostomy tube is to be used, it should not exceed Size 4 (9.4mm OD)
Figure 6: Dimensions of cricothyroid membrane: Range & mean values in millimetres 1
Needle cricothyrotomy
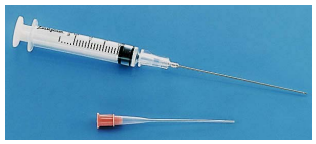
Needle cricothyrotomy using a 12 or 14-gauge cannula(Figure 7) is only employed as an interim measure in an extreme emergency when one is unable to do an open cricothyroidotomy, and in children.
Figure 7: Example of intravenous cannula with needle removed from cannula
Ventilation may be effective if the cannula is attached to high pressure jet ventilation. Ventilation is controlled with a hand-operated jet injector (Figure 8) attached to central wall oxygen, tank oxygen, or the fresh gas outlet of an anaesthesia machine; or may be controlled with the oxygen flush valve of an anaesthesia machine.
However such ventilation via needle cricothyrotomy will only suffice for approximately 45mins as it does not permit adequate ventilation and hence leads to an accumulation of CO2; this can be particularly deleterious for head injury patients as hypoventilation causes raised intracranial pressure. Adult patients must therefore be either intubated or cricothyroidotomy or formal tracheostomy done within 45 minutes.
Should jet ventilation not be available, one would attach either a ventilator or an ambubag to the cannula. However ventilationwith a low-pressure self-inflating resuscitation bag is ineffectivewithin a minute or so.
The cannula can be attached to an ambubag or ventilator in two simple ways:
Fit a 2 or 3ml syringe to the cannula with plunger removed; insert the connection piece of a 7.5mm ID endotracheal tube into the barrel of the syringe (Figure 9)
Fit a 10ml plastic syringe to the cannula with plunger removed; insert an endotracheal tube into the barrel of the syringe and inflate the cuff (Figure 10)
Figure 9: Connection piece of 7.5mm endotracheal tube attached to barrel of 2 or 3ml syringeFigure 10: Insert an endotracheal tube into the barrel of a syringe and inflate the cuff
Complications of needle cricothyrotomy include pneumothorax, subcutaneous and mediastinal emphysema, bleeding, oesophageal puncture, and respiratory acidosis due to hypoventilation. Complete upper airway obstruction proximal to the cricothyrotomy is a contraindication to needle cricothyrotomy because of the risk of causing barotrauma to the lungs. Long term complications include subglottic stenosis and vocal cord injury.
Needle cricothyrotomy: Surgical steps
Position the patient supine with neck exposed and extended (if possible)
Identify surface landmarks i.e. thyroid cartilage, cricoid cartilage and cricothyroid membrane
Prepare a sterile field
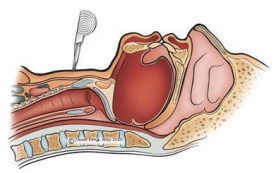
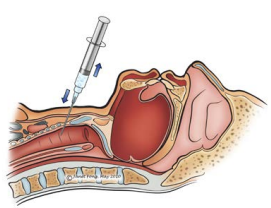
Inject 1% lidocaine with 1:100 000 epinephrine into the skin and through the cricothyroid membrane into the airway to anaesthetise the airway and suppress the cough reflex (if time to do so)
Fix the thyroid cartilage with the 1st & 3rd fingers of the non-dominant hand leaving the 2nd finger free to locate the cricothyroid membrane
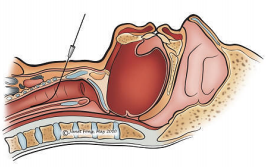
With the dominant hand, pass a 14-gauge intravenous cannula attached to a syringe filled with normal saline, through the cricothyroid membrane, directing it caudally at 450(Figure 10). Bending the distal part of the needle can assist with directing the catheter along the tracheal lumen (Figure 11)
Figure 10: Fix the larynx and insert intravenous cannula at 45Figure 11: Cannula has been bent for easier access
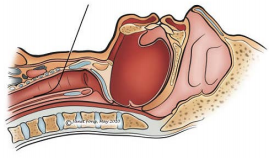
Apply negative pressure to the syringe as the needle is advanced. Air bubbles will appear in the fluid-filled syringe as the needle traverses the membrane and enters the trachea (Figure 12)
Figure 12: Air bubbles appear in the fluidfilled syringe as the needle traverses cricothyroid membrane 4
Advance the cannula and then retract the needle
Attach jet ventilation and ventilate at 15 L/min
Judge the adequacy of ventilation by movement of the chest wall and auscultation for breath sounds, and by pulse oximetry
Open Surgical Cricothyroidotomy
Preoperative evaluation
Level of obstruction: Cricothyroidotomy will not bypass obstruction in the trachea or bronchial tree
Coagulopathy: Unless an emergency, a coagulopathy should be corrected prior to the procedure
Surface anatomy of the neck: Are the relevant landmarks palpable?
Preoperative preparation
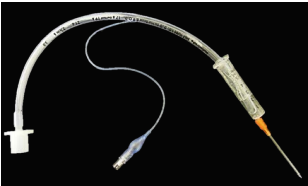
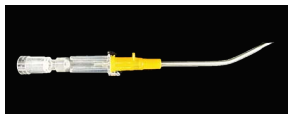
Prepacked cricothyroidotomy kits are available, both for patients requiring airway support (Figure 13) and for patients requiring access for suctioning excessive secretions (Figure 14). However in an emergency airway situation no. 11 or 15 surgical blades, knife handle, curved artery forceps and thin endotracheal tube will do.
Figure 13: Cricothyroidotomy kit for patients requiring airway support and ventilation: Small cuffed tra-cheostomy tube, syringe, scalpel, T-piece, lubricant gel, suture, tracheostomy tapeFigure 14: Mini-tracheostomy kit for patients only requiring lavage and suctioning of secretions: 4mm uncuffed tracheostomy tube with introducer, scalpel, tracheostomy tape, connector piece and suction tubing
Open surgical cricothyroidotomy: Surgical steps
Position the patient supine with anterior neck exposed and extended (if possible)
Identify the surface landmarks i.e. thyroid cartilage, cricoid cartilage and cricothyroid membrane
Prepare a sterile field
Inject 1% lidocaine with 1:100 000 epinephrine into the skin, soft tissue and through the cricothyroid membrane into the airway to anaesthetise the airway (if there time)
Fix the thyroid cartilage with the 1st and 3rd fingers of the non-dominant hand leaving the 2nd finger free to palpate the cricothyroid membrane
If the surface anatomy is well defined use the dominant hand to make a 1-2cm transverse stab incision with a scalpel directly over and right through the cricothyroid membrane at the superior margin of the cricoid (Figure 15). In the more thickset patient, make a 3cm vertical midline incision extending inferiorly from the thyroid prominence (Figure 15); dissect bluntly down to the cricothyroid membrane with the non-dominant index finger; move the finger from side-to-side to clearly feel the cricothyroid membrane
Figure 15: Horizontal or vertical skin incision
Make a 1cm transverse incision through the cricothyroid membrane along the superior edge of the cricoid, angling the scalpel cephalad so as to avoid injuring the vocal cords; await a distinct “pop” sensation as the scalpel pierces through the membrane and enters the larynx; the thick cricoid lamina is located directly posteriorly (Figures 3, 4)
Dilate the tract by passing a curved haemostat through the incision, angling it caudad through the cricoid ring and along the trachea taking care not to perforate the posterior wall of the trachea (Figure 4); alternatively insert a bougie through the tract into the airway
Insert a tracheostomy or endotracheal tube (<7mm ID), either directly or by railroading it over the bougie
If using a cuffed tube, inflate the cuff with air
Commence ventilation
Confirm correct placement of the tube by observation of movement of the chest, auscultation, and end-tidal CO2 if available
Secure the tracheostomy tube by suturing it to skin and/or tracheal tape secured around the neck (Figure 16)
Figure 16: Tracheostomy tube secured with Velcro tape
Percutaneous Cricothyroidotomy using Seldinger Technique
Percutaneous cricothyrotomy using a Seldinger technique requires a needle with dilator and guide wire (Figure 17).
Position the patient supine with neck exposed and extended (if possible)
Identify surface landmarks i.e. thyroid cartilage, cricoid cartilage and cricothyroid membrane
Prepare a sterile field
Inject 1% lidocaine with 1:100 000 epinephrine into the skin and through the cricothyroid membrane into the airway to anaesthetise the airway and suppress the cough reflex (if time to do so)
Fix the thyroid cartilage with the 1st & 3rd fingers of the non-dominant hand leaving the 2nd finger free to locate the cricothyroid membrane
With the dominant hand, make a small stab incision in the skin with a scalpel over the cricothyroid membrane (Figure 18)
Figure 18: Stab incision over cricothyroid membrane4
Pass a finder needle attached to a syringe filled with normal saline, through the cricothyroid membrane, directing it caudally at 450(Figure 19)
Apply negative pressure to the syringe as the needle is advanced. Air bubbles will appear in the fluid-filled syringe as the needle traverses the membrane and enters the trachea
Disconnect the syringe from the finder needle and insert the guide wire through the needle (Figure 20)
Figure 19: Pass needle through cricothyroid membrane 4Figure 20: Insert guide wire through the needle 4)
Retract and remove the needle once the guide wire has been advanced into the airway (Figure 21)
Figure 21: Remove the needle leaving guide wire in place4
Pass the dilator and tracheostomy tube over the guide wire
Jointly advance the dilator and tracheostomy tube over the guide wire into the airway (Figure 22)
Figure 22: Jointly advance dilator and tracheostomy tube over guide wire4
Remove both dilator and guide wire leaving the tracheostomy tube in situ(Figure 23)
Figure 23: Tracheostomy tube in place 4
Secure the tracheostomy tube with tracheostomy tape
Early Complications
Bleeding
Paratracheal false tract: Inadvertent extratracheal placement of the tracheostomy tube can be fatal. It is recognised by the absence of breath sounds on auscultation of the lungs, high ventilatory pressures, failure to ventilate the lungs, hypoxia, absence of expired CO2, surgical emphysema, and an inability to pass a suction catheter down the bronchial tree, and on chest X-ray
Posterior tracheal wall perforation into oesophagus
Pneumothorax, surgical emphysema
Hypercarbia and barotrauma
Late Complications
Glottic or subglottic stenosis due to perichondritis and fibrosis of cricoid
Dysphonia
Persistent stoma
Tracheoesophageal fistula
Postoperative care
Pulmonary oedema:This may occur following sudden relief of airway obstruction and reduction of high intraluminal airway pressures. It may be corrected by CPAP or positive pressure ventilation.
Respiratory arrest:This may occur immediately following insertion of the tracheostomy tube, and is attributed to the rapid reduction in arterial pCO2 following restoration of normal ventilation, and hence loss of respiratory drive.
Humidification:A tracheostomy bypasses the nose and upper aerodigestive tract which normally warms, filters, and humidifies inspired air. To avoid tracheal desiccation and damage to the respiratory cilia and epithelium, and obstruction due to mucous crusting, the tracheostomy patient needs to breathe humidified warm air by means of a humidifier, heat and moisture exchange filter, or a tracheostomy bib.
Pulmonary Toilette: The presence of a tracheostomy tube and inspiration of dry air irritates the mucosa and increases secretions. Tracheostomy also promotes aspiration of saliva and food as tethering of the airway prevents elevation of the larynx during swallowing. Patients are unable to clear secretions as effectively as tracheostomy prevents generation of subglottic pressure, hence making coughing and clearing secretions ineffective; it also disturbs ciliary function. Therefore secretions need to be suctioned in an aseptic and atraumatic manner.
Cleaning tube:Airway resistance is related to the 4th power of the radius with laminar flow, and the 5th power of the radius with turbulent flow. Therefore even a small reduction of airway diameter and/or conversion to turbulent airflow as a result of secretions in the tube can significantly affect airway resistance. Therefore regular cleaning of the inner cannula is required using a pipe cleaner or brush.
Securing tube:Accidental decannulation and failure to quickly reinsert the tube may be fatal. This is especially problematic during the 1st 48hrs when the tract has not matured and attempted reinsertion of the tube may be complicated by the tube entering a false tract. Therefore the tightness of the tracheostomy tapes should be regularly checked.
Cuff pressure: When tracheostomy tube cuff pressures against the tracheal wall mucosa exceed 30cm H20, mucosal capillary perfusion ceases, ischaemic damage ensues and tracheal stenosis may result. Mucosal injury has been shown to occur within 15 minutes. Therefore cuff inflation pressures of >25cm H20 should be avoided. A number of studies have demonstrated the inadequacy of manual palpation of the pilot balloon as a means to estimate appropriate cuff pressures.
Measures to prevent cuff-related injury include:
Only inflate the cuff if required (ventilated, aspiration)
Minimal Occluding Volume Technique: Deflate the cuff, and then slowly reinflate until one can no longer hear air going past the cuff with a stethoscope applied to the side of the neck near the tracheostomy tube (ventilated patient)
Minimal Leak Technique: The same procedure as above, except that once the airway is sealed, slowly to withdraw approximately 1ml of air so that a slight leak is heard at the end of inspiration
Pressure gauge: Regular or continuous monitoring of cuff pressures
References
Dover K, Howdieshell TR, Colborn GL. The dimensions and vascular anatomy of the cricothyroid membrane: relevance to emergent surgical airway access. Clin Anat. 1996;9(5):291-5
Bennett JD, Guha SC, Sankar AB. Cricothyrotomy: the anatomical basis. J R Coll Surg Edinb. 1996 Feb;41(1): 57-60
Little CM, Parker MG, Tarnopolsky R. The incidence of vasculature at risk during cricothyroidostomy. Ann Emerg Med. 1986 Jul;15(7):805-7
Johan Fagan MBChB, FCORL, MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town
South Africa johannes.fagan@uct.ac.za