Buccal mucosa cancers are common in the South Asian subcontinent due to the habit of chewing tobacco, betel quid and betel nut while they account for 5-10% of all oral cavity cancers in North America and Western Europe. Oral cavity cancer has a global incidence of 5.5 Age-standardized rate (ASR) and ranks 11th amongst men (GLOBOCAN 2012).
Surgery is the mainstay of treatment with adjuvant therapy reserved for high risk histological features. Surgical management of buccal mucosa is complex in view of its proximity to the infratemporal fossa and the mandible. A detailed understanding of the anatomy, relations and patterns of tumour spread is essential due to implications relating to oral function, cosmesis and local recurrence.
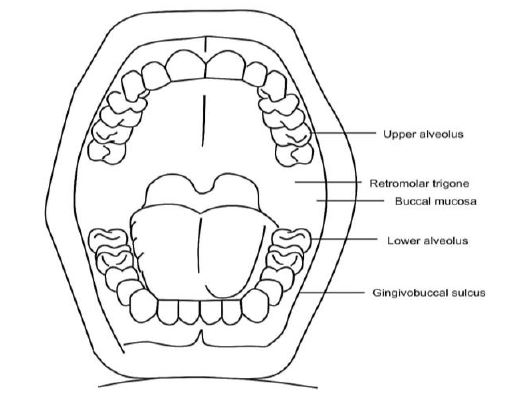
The gingivobuccal complex is a broad term and encompasses the following subsites listed in the International Coding of Diseases (ICD) 10 (Figure 1)
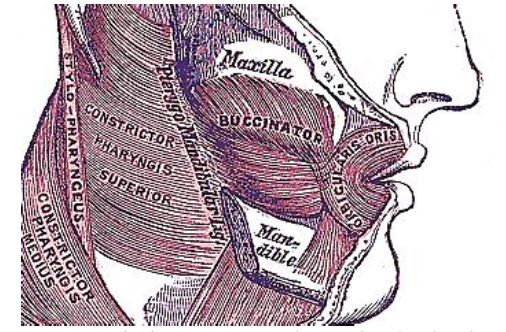
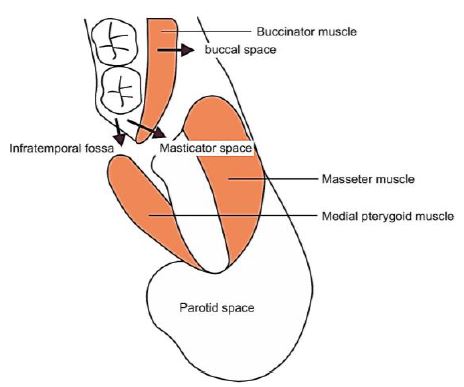
The buccal mucosa lines the inner aspect of the cheek and the lip. It is limited superiorly and inferiorly by its attachments to the alveoli. It extends posteriorly to the retromolar trigone. Deep to the buccal mucosa is the buccinator muscle (Figures 2, 3). Immediately lateral to the buccinator muscle is the facial artery and the buccal artery and the vascular plexus that the buccinator myomucosal flap is based on. (See chapter: Buccinator myomucosal flap)
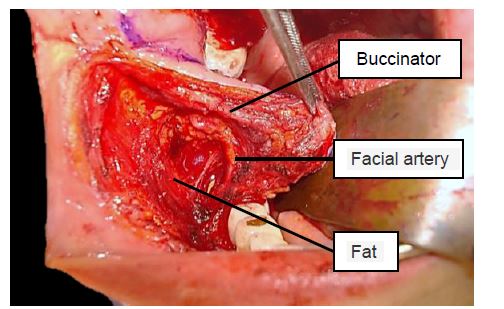
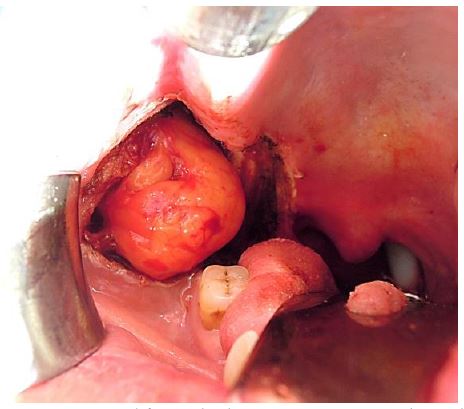
Lateral to the buccinator muscle is the buccal space that contains fat which is traversed by the terminal branches of the facial nerve, and further posteriorly, the buccal fat pad, the zygomaticus major, the subcutaneous tissue and the skin (Figures 3, 4).
The gingival mucosa overlies the alveolus from the point of abutment of the gingivobuccal sulcus to the floor of the mouth. The alveolus is the tooth-bearing area of the mandible and maxilla. It has an outer cortex and has inner trabeculae (medullary bone). The cortical lining of the dental socket is the lamina dura.
The retromolar trigone is a triangular area of mucosa overlying the ascending ramus of mandible. It extends from behind the 3rd molar up to the maxillary tuberosity (Figure 5).
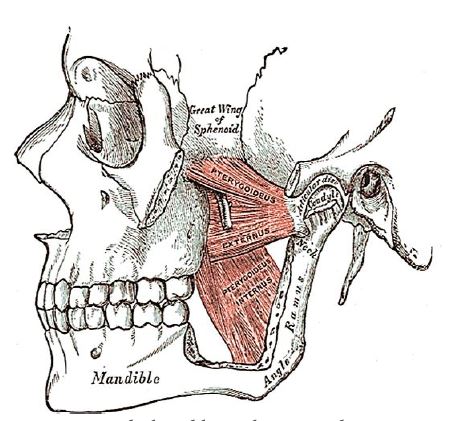
Posteriorly the buccal mucosa is closely related to the medial pterygoid and masseter muscles i.e. the masticator space and the infratemporal fossa. Tumours, particularly from the retromolar trigone, spread to these spaces (Figure 5).
Posterior to the retromolar trigone is the pterygomandibular raphe; it extends between the pterygoid hamulus and the posterior end of the mylohyoid ridge of the mandible (Figure 2). The pterygomandibular space is enclosed by this raphe anteriorly and the medial pterygoid and ascending ramus of mandible on either side, and contains the lingual and alveolar nerves. Posteriorly it is related to the parapharyngeal space.
Stenson’s duct opens in the buccal mucosa adjacent to the 2nd upper molar tooth after crossing the masseter muscle and passing through the buccinator muscle (Figure 6).
gingival mucosa overlies the alveolus from the point of abutment of the gingivobuccal sulcus to the floor of the mouth. The alveolus is the tooth-bearing area of the mandible and maxilla. It has an outer cortex and has inner trabeculae (medullary bone). The cortical lining of the dental socket is the lamina dura.
The retromolar trigone is a triangular area of mucosa overlying the ascending ramus of mandible. It extends from behind the 3rd molar up to the maxillary tuberosity (Figure 5).
Posteriorly the buccal mucosa is closely related to the medial pterygoid and masseter muscles i.e. the masticator space and the infratemporal fossa. Tumours, particularly from the retromolar trigone, spread to these spaces (Figure 5).
to the buccinator muscle is the buccal space that contains fat which is traversed by the terminal branches of the facial nerve, and further posteriorly, the buccal fat pad, the zygomaticus major, the subcutaneous tissue and the skin (Figures 3, 4).
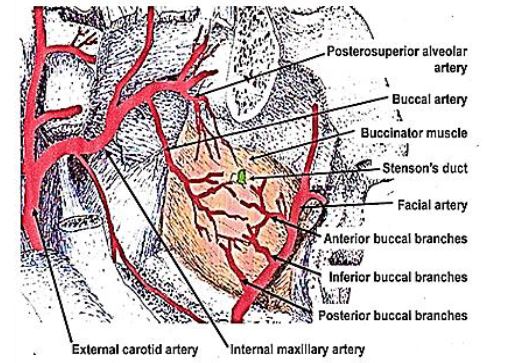
Arterial supply (Figure 6): The buccal mucosa is supplied by the facial and buccal arteries; the buccal artery originates from the pterygoid branch of the maxillary artery. The inferior alveolar artery is a branch of the mandibular branch of the maxillary artery and enters the mandibular canal to supply the inferior alveolus. The superior alveolus is supplied by the posterior superior alveolar artery, a branch of the pterygopalatine segment of the maxillary artery.
Venous drainage: The pterygoid plexus drains into the facial vein which eventually drains into the internal jugular vein.
Lymphatics: The buccal mucosa drains into the deep cervical nodes. Level IB (submandibular nodes) is the first echelon of lymphatic spread of tumour.
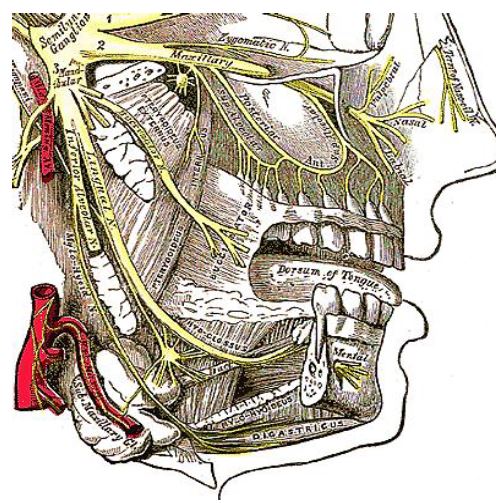
Innervation: (Figures 7, 8) Sensory supply is via the maxillary and mandibular divisions of the trigeminal nerve. Motor supply to the muscles of mastication is by the mandibular nerve; the buccinator muscle is innervated by the buccal branch of the facial nerve.
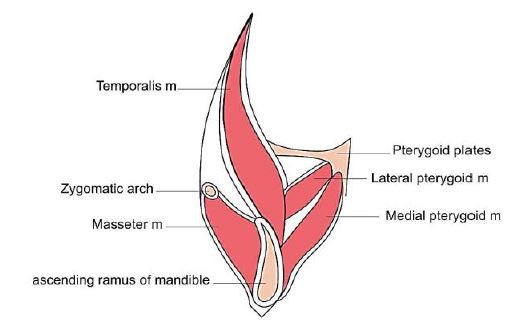
Masticator space (Figure 9)
Enclosed within superficial layer of deep cervical fascia covering muscles of mastication
Inferior boundary: Lower border of mandible
Superior boundary: Parietal calvarium
Medial boundary: Fascia medial to medial pterygoid muscle
Lateral boundary: Fascia overlying masseter and temporalis muscles
Contents: Muscles of mastication, internal maxillary artery, mandibular nerve
Clinical relevance: Involvement of masticator space is considered to be locally very advanced disease i.e. T4b stage (AJCC/TNM)
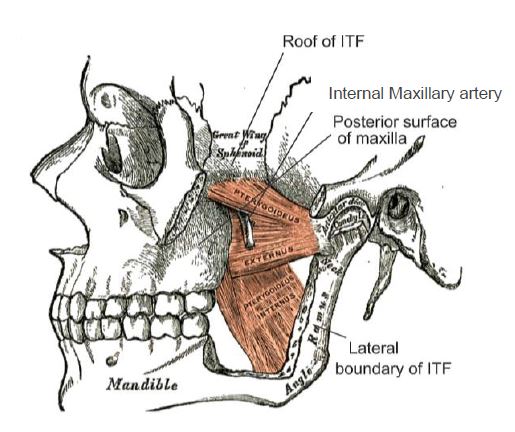
Infratemporal fossa/ITF (Figure 10)
Medial boundary: Lateral pterygoid plate of sphenoid bone
Lateral boundary: Mandible
Superior boundary: Greater wing of sphenoid bone and squamous part of temporal bone
Inferior boundary: Medial pterygoid muscle
Anterior boundary: Posterolateral wall of maxilla
Posterior boundary: Tympanic part of temporal bone
Relations: Inferior orbital fissure, pterygomaxillary fissure
Contents: Lower part of temporalis muscle, part of masseter, medial and lateral pterygoid muscles, internal maxillary artery, pterygoid venous plexus, branches of mandibular nerve, facial nerve and otic ganglion
Clinical relevance: ITF involvement can be either “high” or “low”. Tumours involving the high ITF (involving lateral pterygoid and temporalis muscles) are considered irresectable because tumour can escape through the pterygomaxillary and inferior orbital fissures making the possibility of complete (R0) resection unlikely
Buccal Space (Figures 3, 4, 6)
Medial boundary: Buccinator muscle
Lateral boundary: Zygomaticus major muscle
Contents: Mainly buccal fat pad which communicates posteriorly with the retroantral fat pad, Stenson’s duct, minor or occasionally accessory salivary glands, facial and buccal arteries, facial vein, and branches of facial and mandibular nerves
Clinical relevance: Tumour infiltration into the buccal space can potentially lead to spread to the infratemporal fossa via the retroantral fat pad
A combination of clinical assessment (under anaesthesia if indicated) and imaging is required to evaluate buccal lesions and to assess resectability and to plan the extent of resection.
Orthopantomogram/Panorex (OPG) is used primarily to assess dentition for dental prophylaxis prior to radiotherapy. It does not yield soft tissue information; it requires a loss of up to 30% of bony cortex to detect mandibular invasion (poor sensitivity); and is not ideal for midline lesions due to superimposition of the spine (Figure 11).

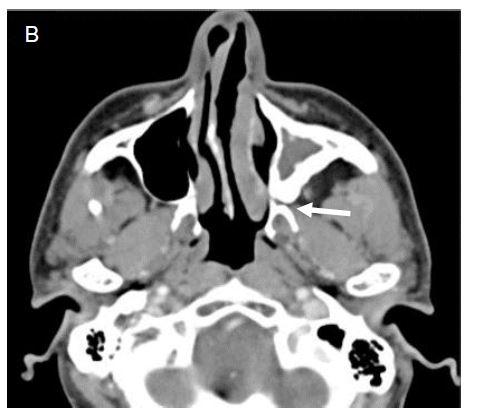
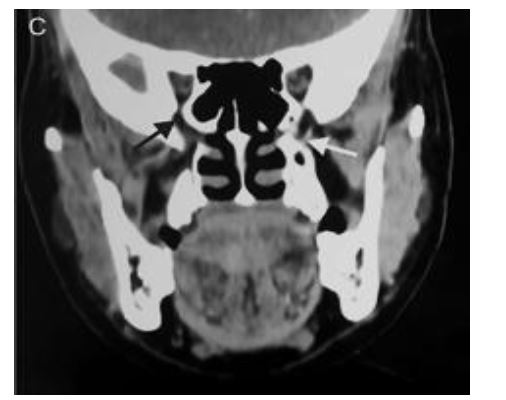
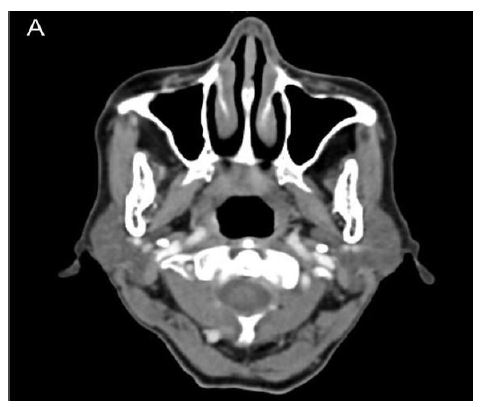
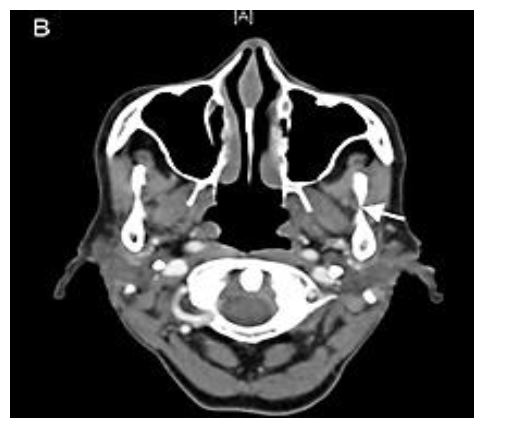
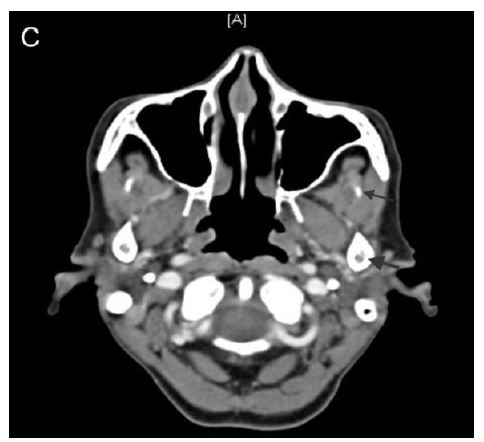
Contrast Enhanced Computed Tomography (CECT) with a “puffed cheek technique” is the preferred imaging modality to assess the primary as well as the neck. A Multidetector CT scan with sagittal reformatting can detect mandibular involvement with an accuracy of up to 90%. Infratemporal fossa involvement is assessed the relationship of tumour to an arbitrary line drawn in an axial plane through the sigmoid notch (between coronoid and condyle) of the mandible (Figure 12). Lesions extending superior to the sigmoid notch are considered irresectable due to involvement of the higher part of the infratemporal fossa.
Magnetic Resonance Imaging (MRI) provides superior soft tissue delineation compared to CT. It is indicated for buccal lesions clinically removed from the bone, to assess involvement of the buccal space and infratemporal fossa. MRI may be required in cases of clinical extension into bone to determine involvement of marrow and inferior alveolar nerve. MRI however tends to overestimate bony involvement and is inferior to CT to assess cortical erosion.
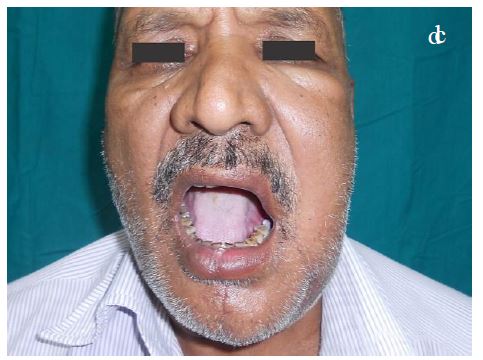
Patients with buccal cancer may have trismus, either longstanding due to oral submucous fibrosis, or of recent onset due to spasm or invasion of the muscles of mastication (mylohyoid, masseter, medial pterygoid, temporalis, and lateral pterygoid). Securing the airway in such patients may require fibreoptic intubation or an awake preoperative tracheostomy. Nasal intubation is preferred so as to remove the airway from the surgical field. The surgeon may elect to pack the throat during tumour excision to avoid aspiration of blood.
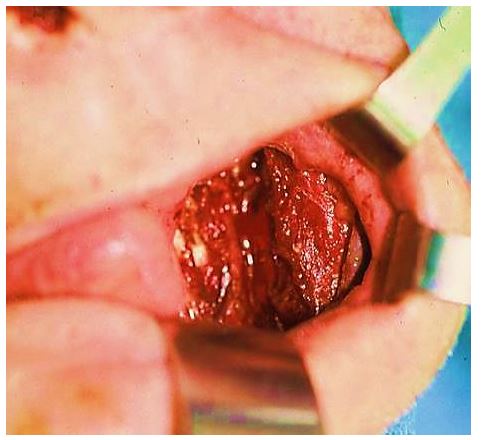
Peroral: Small anterior lesions are accessible without an external incision (Figure 13).
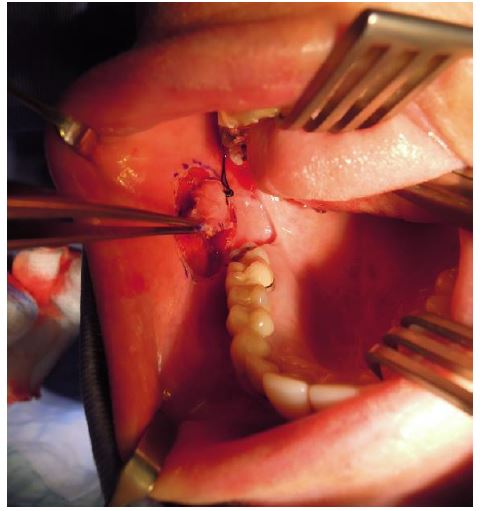
However a peroral approach should be avoided in posterior lesions even if they are small. It is pertinent to resect an adequate base with wide margins as the base is the commonest site of compromised margins with peroral excision. Occasionally an anterior lesion requiring marginal mandibulectomy can be approached perorally.
Cheek flap: Most lesions of the buccal mucosa (with above exceptions) are approached via a cheek flap with one of the two incisions described below.
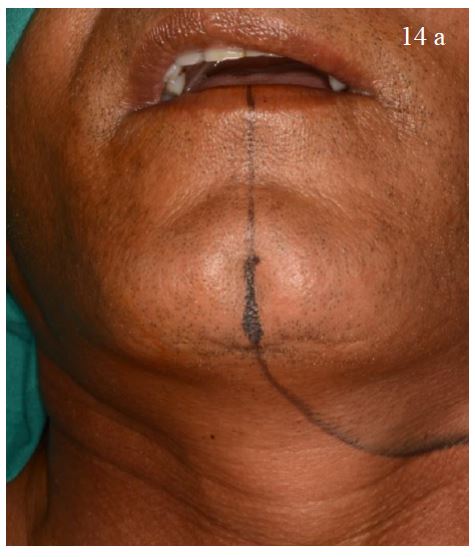
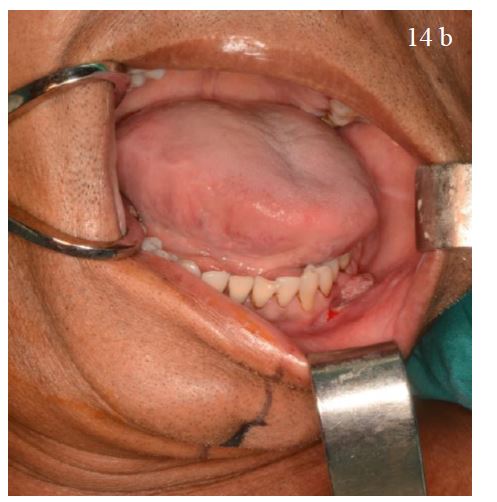
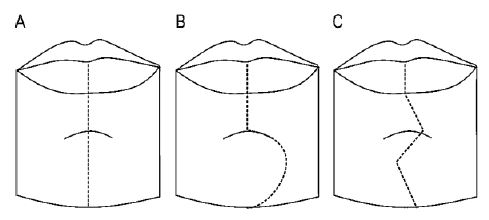
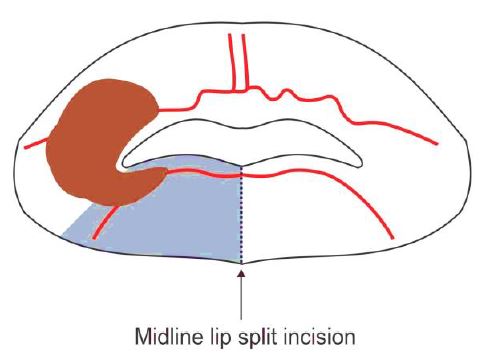
Midline lip split: When a lesion is located away from the oral commissure, the lip is split in the midline. This incision maintains better oral competence. The incision is continued over the mentum, curving towards the hyoid up to the mastoid process along a suitable skin crease at least 2 finger breadths below the mandible (Figure 14). The midline lip split incision can be modified for better cosmesis (Figure 15). (Editor favours straight incision as in Figure 15A).
Angle split: The incision is made at the oral commissure when the lesion approaches close to the commissure. This avoids devascularising the lip segment between the commissure and the midline. It is also preferred when adjacent skin excision is required (Figure 16).
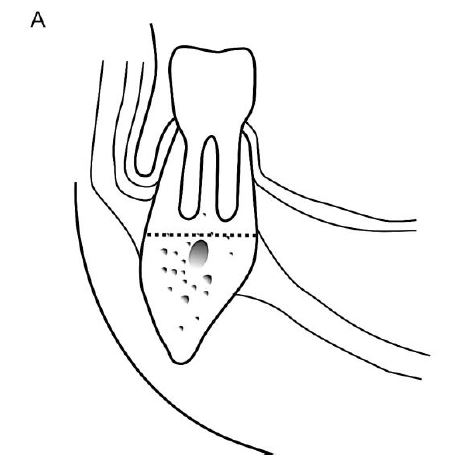
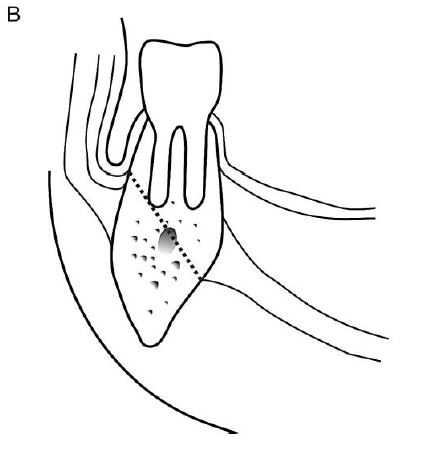
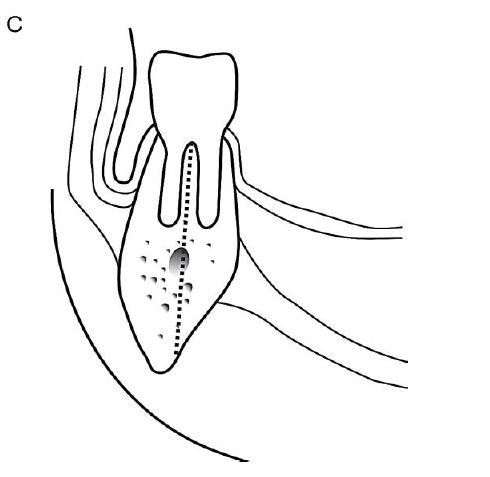
Periosteum is a robust barrier to bone invasion. In alveolar lesions with intact dentition, the mandible is generally invaded via its occlusal surface (Figures 11, 17). In the retromolar trigone or in edentulous mandibles, the occlusal surface corresponds to the junction of the attached and reflected mucosa (point of abutment). In irradiated mandibles and in large tumours, the mandible can be invaded at multiple points due to multiple breaks in the periosteum.

With cancers of the floor of the mouth, mandible is infiltrated at the point of abutment. Hence a horizontal marginal mandibulectomy can be attempted in early gingivobuccal complex cancers lesions to include invasion at the occlusal surface; floor of mouth cancer requires vertical or oblique marginal mandibulectomy to completely excise the lingual plate due to invasion occurring directly at the point of abutment.
Marginal mandibulectomy is indicated when tumour abuts mandible without gross invasion, or when there is only superficial bony invasion.
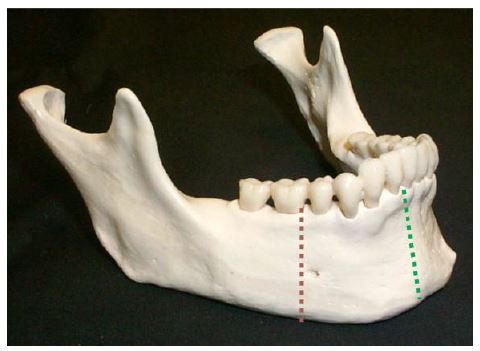
Three types of marginal mandibulectomy are described i.e. horizontal, vertical and oblique (Figure 18). As the lingual plate is weaker than the buccal plate, an isolated buccal plate excision may not withstand subsequent weight bearing and the bone may fracture. Hence isolated buccal plate excision is risky in buccal mucosa lesions.
The theory of preferential route of tumour entry through the inferior alveolar nerve has been refuted by multiple studies; hence it is no longer advocated to include the inferior alveolar nerve up to the skull base with a rim resection.
Adequate exposure is achieved with a lower cheek flap. Occasionally, a small anterior lesion can be approached perorally (Figure 19).

After the mucosal and soft tissue incisions have been made, bone cuts are marked corresponding to the soft tissue incisions (Figure 20).
The edges of the bone should be “canoe shaped” to avoid sharp corners (Figure 21).
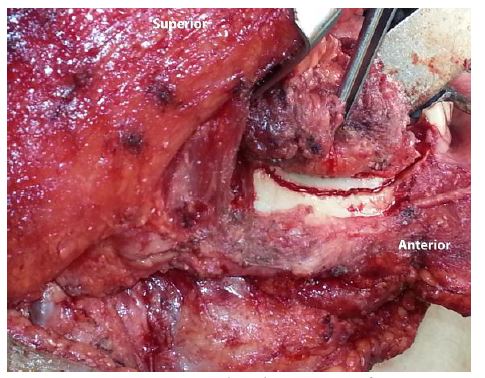

Right-angled cuts predispose to stress fractures and hence are avoided. Inferiorly a bony bridge of >1cm in height should be retained to avoid a stress fracture. The bone is cut with sharp bone-cutting instruments e.g. a powered saw. Finally the corresponding gingivolingual sulcus is divided to deliver the specimen.
With marginal mandibulectomy for retromolar trigone cancer, the anterior aspect of the ascending ramus of the mandible is excised in continuity with the coronoid process, as releasing the attachment of the temporalis muscle avoids postoperative trismus.
This is indicated when there is gross bone erosion, either clinically or radiologically; for significant paramandibular disease; for postradiotherapy recurrence due to the multiple routes of tumour entry; or with a pipe stem mandible (inadequate bony remnant of <1cm in height) (Figure 22).
Segmental mandibulectomy may encompass the mandibular arch (mid-third segment) or may be arch-preserving (lateral segment). Mandibulectomy that includes the entire ascending ramus, condyle and coronoid can either be a posterior segmental mandibulectomy (posterior to mental fora-men) or hemimandibulectomy (Figure 23).

Because intubation may be challenging in the presence of trismus, the surgical team must be present during induction of anaesthesia. If a difficult intubation is anticipated, then one should infiltrate the skin and trachea with local anaesthesia and a vasoconstrictor prior to induction, and the tracheostomy team must be ready to proceed if necessary. The alternative is to perform an awake tracheostomy before induction of anaesthesia. In cases where intubation is straightforward, the decision whether to do an elective tracheostomy at the end of the procedure is a judgement call of the surgeon and anaesthetist. However one should have a low threshold for tracheostomy. (See chapter: Tracheostomy)
If a neck dissection is to be done, then Levels 1 and 2 are dissected before resecting the primary. This facilitates resection of the primary tumour; it allows the pathologist to do frozen sections of the resected tumour; and for the reconstructive surgeon to examine the surgical defect and raise a flap while the neck dissection is completed. The submandibular gland may be kept in continuity with the main specimen after ligating the facial artery where it exits behind the posterior belly of digastric, should the tumour be involving the lingual surface of the mandible or the floor of the mouth. Supraomohyoid neck dissection (Levels 1-3) is used as an elective neck dissection for buccal cancer. In the presence of nodal metastasis, either Levels 1-4, or Modified Neck Dissection (Levels 1-5) is done. (See chapters: Selective neck dissection technique and Modified and radical neck dissection technique).
Once Levels 1 & 2 of the neck dissection have been competed, a decision is made about whether to do a midline lip split or an angle split incision. The lower cheek flap is raised in a subcutaneous plane keeping adequate soft tissue on the tumour. The mucosal cuts are made with adequate margins.
After incising the mucosa around and soft tissue using diathermy or a knife, bone cuts are marked adjacent to the soft tissue. The posterior mucosal cut is made according to the extent of tumour. Attention should be paid mainly to the 3rd dimension i.e. deep resection margin. This margin must contain at least one layer of normal tissue beyond the tumour. With this in mind, it should contain the buccinator muscle with superficial lesions and the buccal fat pad or the zygomaticus major muscle with deeper lesions. With lesions deeper than that e.g. adhering to skin or causing peau d’orange, the overlying skin is excised to achieve an adequate margin.
Bone resection depends on whether marginal, segmental or hemimandibulectomy is required. Marginal mandibulectomy is illustrated in Figures 18-21.
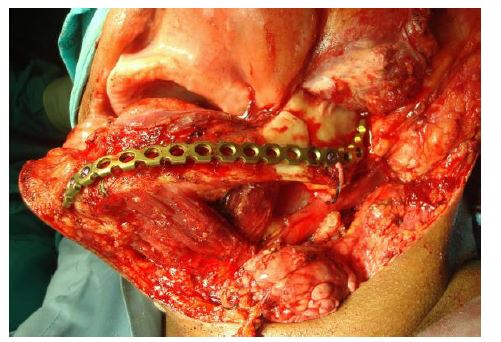
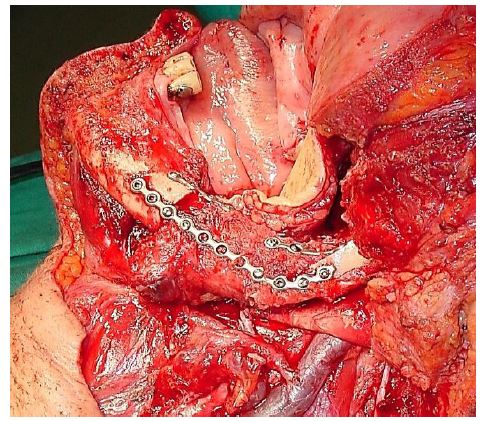
The following description applies to a segmental or hemimandibulectomy. A vertical osteotomy is made about 2cms anterior to the tumour with a powered saw, drill or Gigli saw. This allows the surgeon to reflect the mandible laterally like opening a book and to expose the tumour. If a bony reconstruction is to be done, then the mandible is preplated to ensure an accurate repair (Figure 24). (See chapter: Vascularised free fibula flap reconstruction).
If the retromolar trigone is not involved, then the posterior osteotomy is made 2cms behind the posterior edge of the tumour (Figure 25).
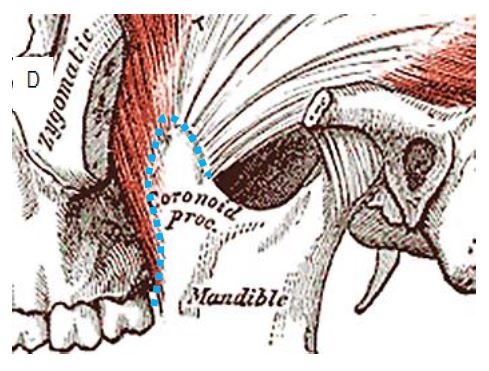
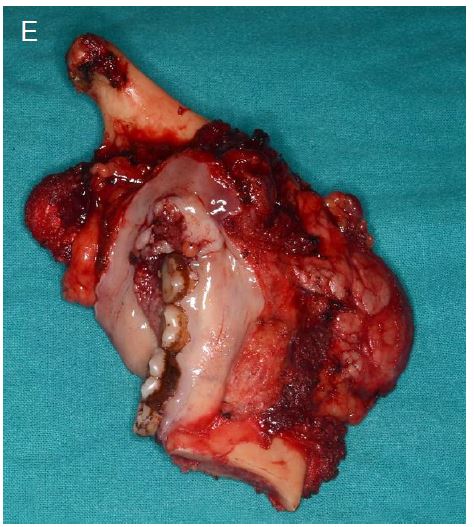
A posterior segmental or a hemimandibulectomy may be required with deep-seated tumours extending posteriorly beyond the retromolar trigone (Figures 26 A-E). The masseter muscle is reflected off the bone or is included with the specimen depending on the extent of the tumour. The coronoid process is exposed and released from its attachment to the temporalis muscle, remaining close to the bone to avoid injuring the vessels medial to the coronoid process.


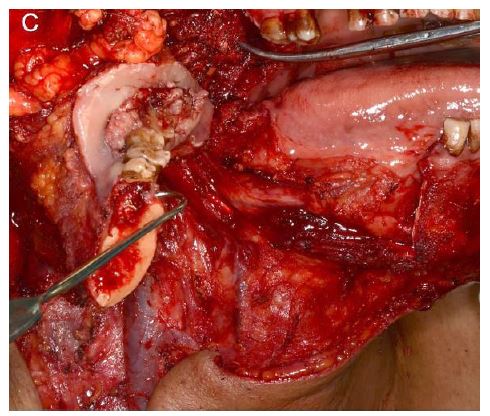
With the mandible now mobile and swung out laterally, the posterior mucosal cuts can be made behind the tumour, cutting through medial pterygoid muscle and its attachments to the lateral pterygoid plate and the maxillary tuberosity, and the inferior alveolar nerve (and lingual nerve) at its entry into the mandibular canal. The maxillary artery may have to be ligated in the sigmoid notch. The mandibular condyle is released from the lateral pterygoid muscle and the hemimandible and tumour are delivered.
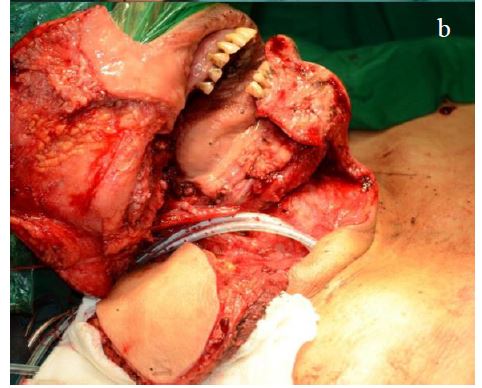
This refers to excision of the superior and inferior alveoli with the intervening interalveolar tissue (like a bite). It is indicated for lesions involving the retromolar trigone extending to the superior alveolus. The specimen consists of the inferior as well as the superior alveolus in continuity with the overlying retromolar trigone mucosa and soft tissue formed by the pterygoid muscles (Figure 27). The bony cuts for the mandibulectomy are as described above.

Mucosal incisions are made on the superior alveolus with adequate margins. The mucosal incision of the inferior alveolus is extended to meet the mucosal incision on the superior alveolus at the retromolar trigone. The superior alveolus is cut with a bone cutting instrument to traverse the posterolateral wall of the maxilla up to the maxillary tuberosity. The location of the posterior bony cut depends on the tumour.
If the lesion does not involve the ITF, then the bone cut is made anterior to the pterygoid plates. However, if the lesion involves the medial pterygoid muscle, the pterygoid plate is included in the specimen to ensure adequate soft tissue resection that includes the pterygoid muscles. “Bite excision” with resection of the entire medial pterygoid muscle is performed when the lower ITF is involved. If resection of the higher ITF is warranted, then “bite excision” encompassing the pterygoid plates is performed to include the entire medial and lateral pterygoid muscles (Figure 28). The temporalis muscle below the temporal fossa is resected in continuity with the coronoid up to the roof of the ITF.
The aims are to restore form and function. Whether to repair a defect depends on its size and depth, and whether there is a through-and-through defect into the neck.
Buccal soft tissue defect only: Small defects can be closed primarily, or left to granulate and heal by secondary intention like a tonsillectomy defect. Larger defects that include resection of the buccinator muscle that are left to granulate may lead to significant trismus due to scarring and contraction of the scar tissue.
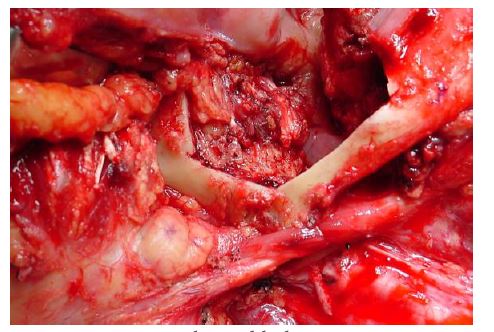
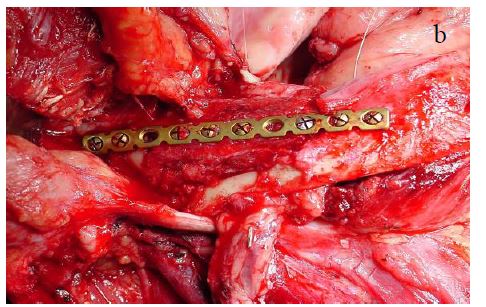
Marginal mandibulectomy: A marginal mandibulectomy defect can be strengthened with an onlay fibula or radial forearm osseocutaneous flap (Figures 29a, b).
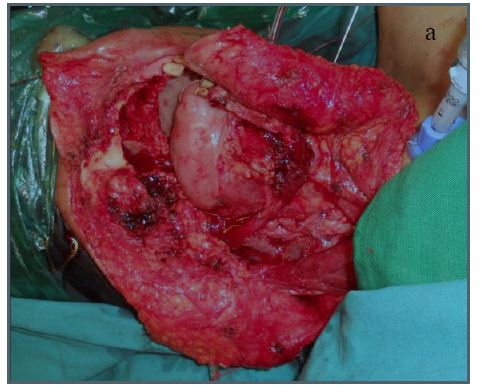
Segmental mandibulectomy: If the resection crosses the midline and includes the mandibular arch e.g. mid-third mandible segment, reconstruction with an osseocutaneous free flap is mandatory to avoid a debilitating Andy Gump deformity (Figure 30).
For lateral and posterior segmental, or hemimandibulectomy defects, reconstructtion with a pectoralis major myocutaneous flap is an acceptable alternative if osseocutaneous free flap reconstruction is not possible, or is inadvisable e.g. in the elderly, frail and unfit.
Large soft tissue defect: A large soft tissue defect following e.g. a “bite excision” or infratemporal fossa clearance can be reconstructed with pedicled flaps (forehead, temporalis, pectoralis major, deltopectoral) or free flaps (radial free forearm, anterolateral free thigh).
Facial skin defect: Skin can be reconstructed by bipaddling a radial free forearm, anterolateral thigh (Figure 31), or pectoralis major flap to provide both inner and external skin cover. Else a double flap i.e. one flap to cover the inner mucosal and soft tissue defect and the other to cover the skin loss, can be used.

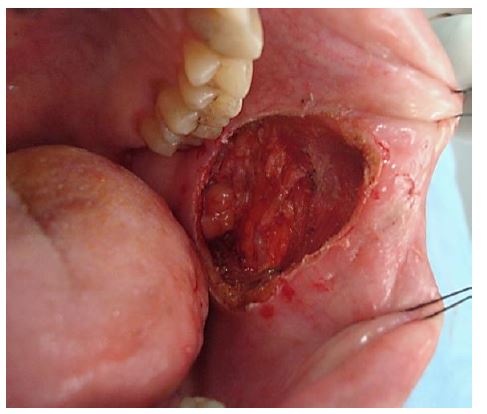
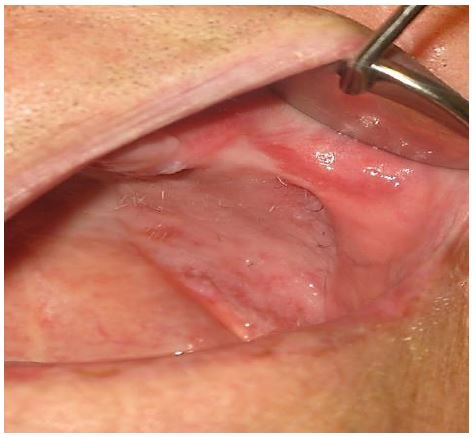
Split skin grafts can be employed for superficial defects. Figure 32 illustrates a typical soft tissue defect following resection of a buccal tumour; this may be closed with a local, pedicled or a free microvascular transfer flap. Free flaps are generally preferred to local or pedicled flaps as they can be better tailored to the defect.
Split skin graft: The graft is harvested from the thigh and the mucosal defect is quilted with the skin graft with absorbable sutures. Pressure is applied to the graft by using a bolus e.g. BIPP impregnated gauze, which is tied over the graft and kept in situ for 5 days. However, using a split skin graft for deeper and larger defects causes fibrosis that may cause trismus.
Buccal fat pad flap (Figure 33): The buccal fat is conveniently located in the posterior part of the buccal space, and can be gently delivered into the defect and used to fill the defect. It subsequently mucosalises. In some cases it may cause a scar band and trismus. (See chapter: Buccal fat pad flap)
Pectoralis major flap (Figure 34): This was the workhorse of oral cavity reconstruction prior to the advent of free microvascular tissue transfer flaps. The pectoralis major flap has a robust blood supply; has a long pedicle length which makes it amenable to reconstruction of a defect as superior as the lower border of the zygoma; the shape of the flap can be adjusted to the shape of the defect; and a large flap can be harvested. It remains a good choice when free flaps are not available, as a salvage procedure for a failed free flaps or when patients cannot tolerate a long procedure e.g. the elderly and infirm. (See chapter: Pectoralis major flap)


Nasolabial flap (Figures 35 a-d): The nasolabial flap has advantages that the donor site is adjacent to the defect, that the flap is thin and pliable and has a robust blood supply that permits shaping of the flap to precisely fill the defect. A larger defect, particularly when located anteriorly, can be covered with bilateral nasolabial flaps. (See chapter: Nasolabial flap for oral cavity reconstruction)

Tongue flap: Advantages are that the flap is harvested adjacent to the defect and that there is insignificant donor site morbidity. Generally a posteriorly-based flap is used. It is a single stage procedure and the donor site is closed primarily.
Temporalis flap: This is favoured by some surgeons. It is based on the deep temporal artery which courses close to the coronoid process of the mandible which this has to be preserved. (See chapter: Temporalis muscle flap)
Forehead flap: It has a robust blood supply, is pliable and the entire forehead can be utilised. It is however associated with significant cosmetic morbidity, and is therefore generally reserved as a 2nd line reconstructtive option.
Deltopectoral flap: It is quick and easy to harvest, has consistent anatomy, and is a pliable flap. For oral cavity repair it generally requires a 2nd stage surgery after 3 weeks to disconnect the pedicle. (See chapter: Deltopectoral flap and cervicodel-topectoral fasciocutaneous flaps for head and neck reconstruction)
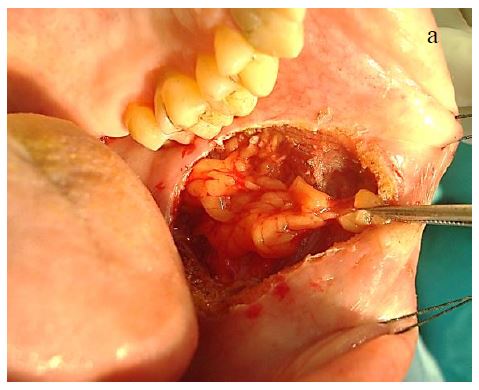
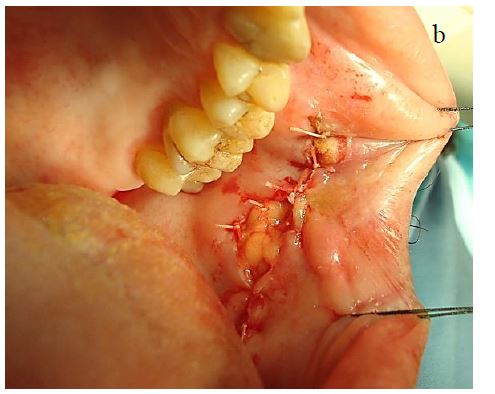
Radial free forearm flap (Figures 36 a-d): It is a thin, pliable flap with a consistent blood supply and a long vascular pedicle. It is quick and easy to harvest. Donor site morbidity is worse than with anterolateral thigh free flaps. Its pliability makes it amenable to reconstruct a variety of oral defects. It can also be harvested as an osseocutaneous flap (Figure 29). Figures 36 a-d illustrate the utility of a radial free forearm flap to reconstruct a defect following “bite” excision.



Anterolateral free thigh flap (Figure 37): It can be harvested with muscle and hence used for larger soft tissue defects. Donor site morbidity is insignificant.


Radial osseocutaneous flap (Figure 29): This can be complicated by fractures of the remaining radius, and restriction of forearm range of movement. Hence it is the authors’ preference to use a free fibula flap.
Free fibula flap (Figure 38): Advantages include long bone length, a segmental blood supply making multiple osteotomies feasible, and minimal donor site morbidity. (See chapter: Vascularised free fibula flap reconstruction)
Scapular flap: This is useful in cases requiring skin, bone as well as muscle based on a single vascular pedicle, and is most commonly used for maxillary and orbital defects.
Airway: Elective tracheostomy is always indicated if mandibular resection crosses the midline with excision of both genial tubercles resulting in the tongue dropping back, extensive composite palatal resection, or buccal mucosal resection requiring reconstruction with a bulky flap.
Position: Maintain the patient at 15 degrees head-high to reduce venous congestion and bleeding. Maintain a head position that avoids twisting of the vascular pedicle of a free flap.
Feeding: Patients are fed by nasogastric feeding tube for at least 5 days, and until that patient is able to tolerate their own saliva.
Antibiotics: A broad spectrum antibiotic is administered for 24 hours.
Jaw stretching exercises: Trismus is one of the commonest and most disabling sequelae of surgery for buccal cancer because of scarring and shortening of the muscles of mastication, as well as scarring in the tumour bed and of the flap or skin graft. Jaw stretching exercises should commence after initial wound healing i.e. about 5-7 days after surgery, and should be continued for a long period of time.
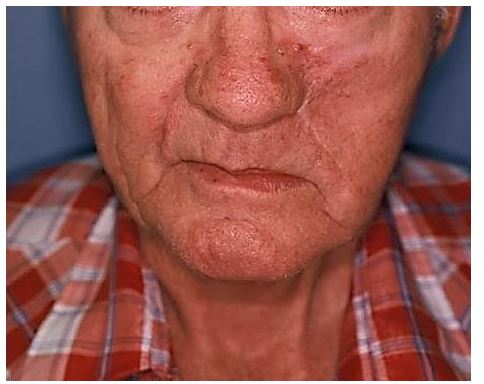
Bite guide prosthesis: Unopposed contraction of the opposite muscles of mastication result in deviation of the lower jaw following hemimandibulectomy (Figure 39).

A bite guide prosthesis prevents this deviation and should be used for at least 6-8 weeks following surgery until complete healing has occurred (Figure 40).

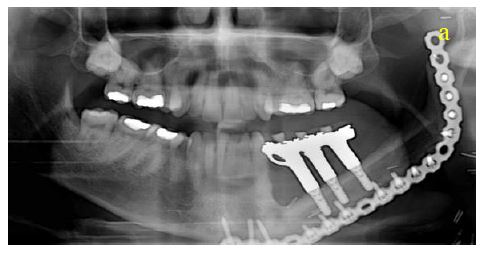
Dental rehabilitation: Dental implants can be considered in cases of free bone transfer (Figures 41a, b) and dentures may have to be adjusted.

Devendra A Chaukar M.S, D.N.B.
Associate Professor
Department of Head and Neck Surgery
Tata Memorial Hospital
Mumbai, India
dchaukar@gmail.com
Mitali Dandekar M.S, D.N.B.
Department of Head and Neck Surgery
Tata Memorial Hospital
Mumbai, India
mitalidandekar@gmail.com
Johan Fagan MBChB, FCORL, MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town
South Africa
johannes.fagan@uct.ac.za