
Neck abscesses can be difficult to drain and have fatal consequences if not timeously diagnosed, accurately localised and promptly incised and drained. Yet the management is commonly left in the hands of surgical trainees.
This chapter presents the relevant surgical anatomy and surgical approaches to the different fascial spaces of the head and neck. Because fascial planes both direct and confine spread of sepsis, it is important to have an understanding of the fascial planes and fascial spaces of the head and neck.
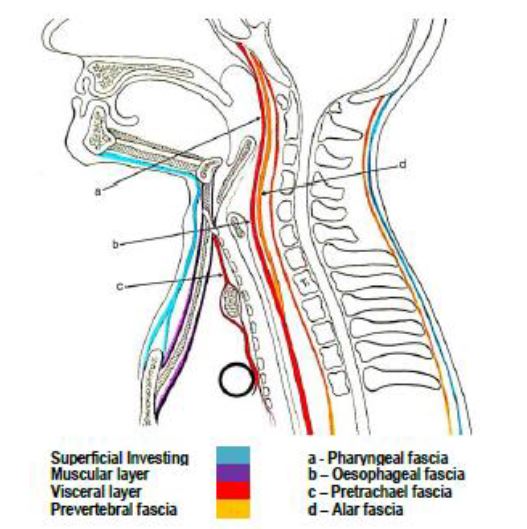
This very thin, delicate fascia is found just deep to the skin and envelopes the muscles of the head and neck including platysma and the muscles of facial expression. It is so thin that it may be difficult to identify when incising the neck. It extends from the epicranium above to the axillae and upper chest below and includes the superficial musculo-aponeurotic system/SMAS. The space deep to the superficial cervical fascia contains fat, vessels (e.g. anterior and external jugular veins), nerves and lymphatics and is by definition not a deep neck space (Figure 1). Abscesses located either superficial to or within the tissue space immediately deep to the superficial cervical fascia are treated by simple incision and drainage.
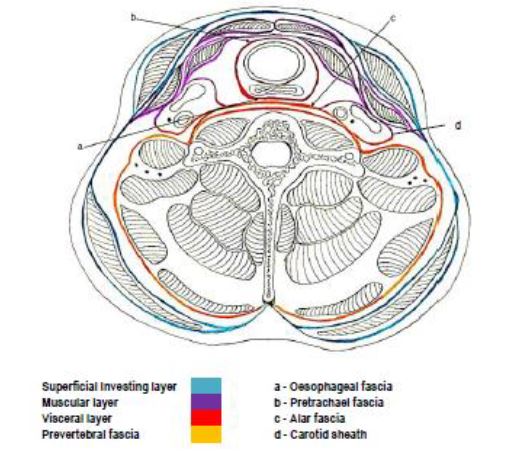
Deep Cervical Fascia (Figures 2-4)
This envelopes the deep neck spaces; hence an understanding of its anatomy is key to managing deep neck sepsis. It comprises 3 layers i.e. superficial, middle, and deep.
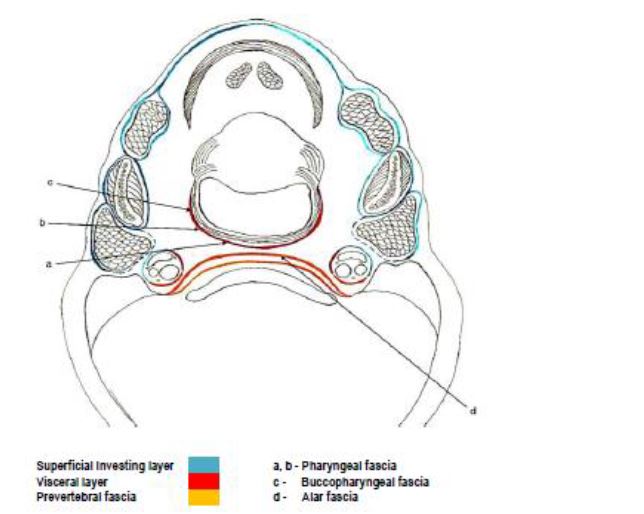
The superficial layer, also known as the investing layer, surrounds the neck and envelopes the muscles of mastication i.e. masseter, buccinator, digastric and mylo-hyoid (Figures 4, 5).
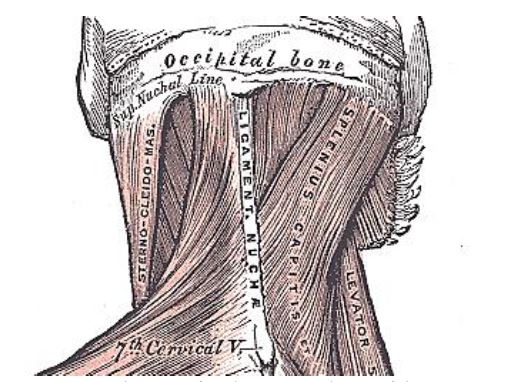
a) Superior nuchal line of occipital bone (Figures 2, 6)
b) Posteriorly merges with ligamentum nuchae, a midline intermuscular extension of the supraspinous ligament (Fig-ures 2, 3, 6)
c) Mastoid processes of temporal bones
d) Zygomatic arches
e) Inferior border of mandible
f) Hyoid bone
g) Manubrium sterni
h) Clavicles
i) Acromion
j) Forms stylomandibular ligament
k) Fascia parts just above manubrium sterni to contain anterior jugular veins, and attaches to anterior and posterior surfaces of the manubrium (Figure 2)
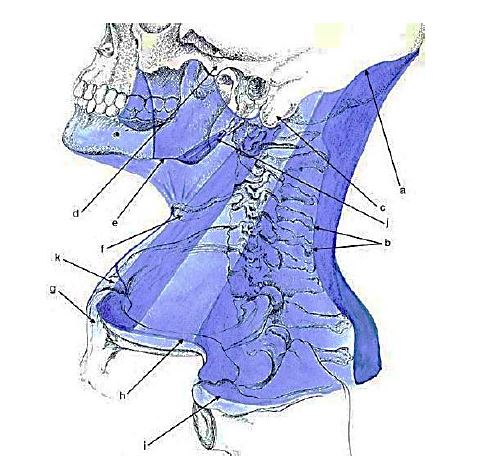
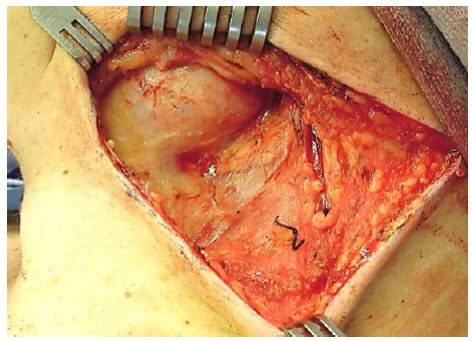
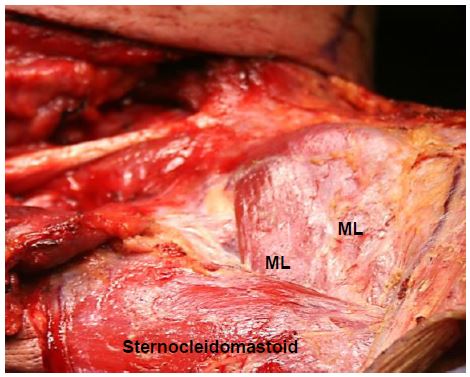
The fascia splits into superficial and deep layers to enclose trapezius and sternoclei-domastoid (Figure 3). It also encapsulates the submandibular and parotid glands (Fig-ures 4, 7, 8), and contributes to the carotid sheath (Figure 3).

Between the ramus of the mandible and the hyoid bone it envelopes the anterior belly of the digastric muscle (Figure 9). The superficial layer of deep cervical fascia therefore defines the parotid, submandibular and masticator spaces and contributes to the wall of the carotid space (Figures 4, 7).
The middle layer of deep cervical fascia extends superiorly from the skull base along the carotid sheath to the pericardium (Figures 2, 3, 10). It has muscular and visceral layers:
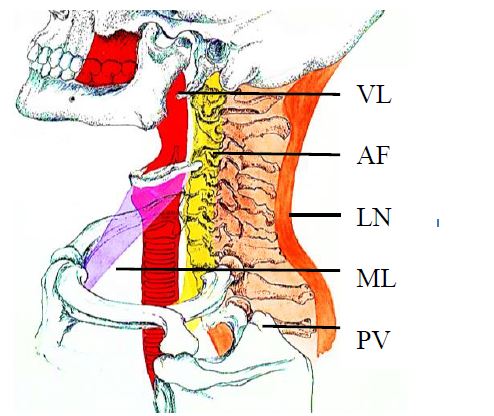
This encircles the prevertebral and para-spinal muscles, and also contributes to the carotid sheath. It is divided into pre-vertebral and alar fasciae.

The deep fasciae create clinically relevant deep neck spaces, some of which inter-connect with one another. Some are potential spaces and become apparent only when distended by pus or air (surgical emphysema). The terminology and classifications of deep neck spaces used in the literature are not entirely consistent.
Working from cephalad-to-caudad the deep neck spaces may be grouped as follows:
I. Facial region
II. Suprahyoid region
III. Infrahyoid region: Pretracheal space
IV. Entire Neck
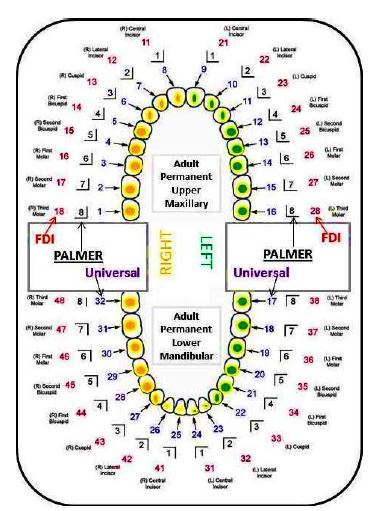
Fascial space infections are often of odontogenic origin. Hence it is important to know how to number the teeth, especially when interpreting radiology reports. Three different numbering systems are used in dentistry (Figure 14).
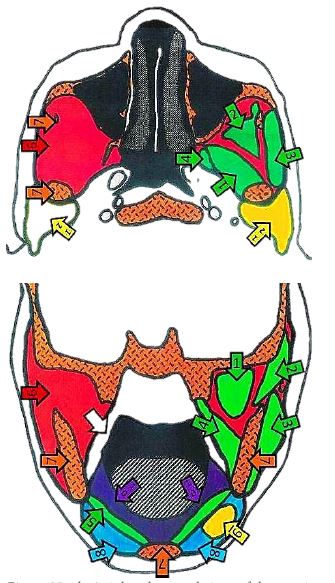
The buccal space is confined laterally by the superficial cervical fascia just deep to the skin, medially by the investing layer of cervical fascia that overlies the buccinator muscle, anteriorly by the labial muscular-ture, posteriorly by the pterygomandibular raphe, superiorly by the zygomatic arch and inferiorly by the lower border of the mandible (Figure 15). It contains buccal fat, Stenson’s duct, terminal branches of the facial nerve, and the facial artery and veins (Figure 16).
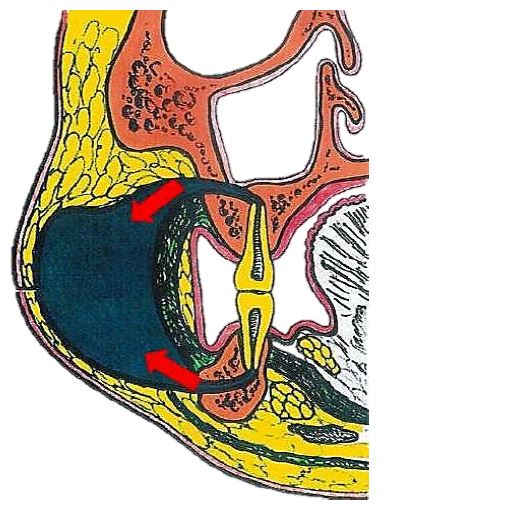
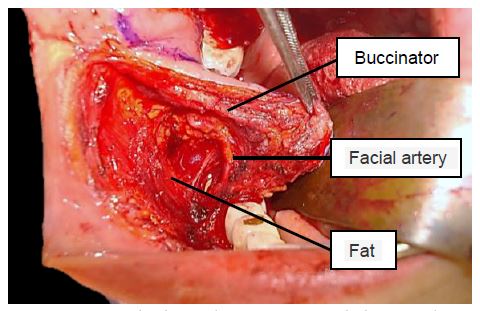
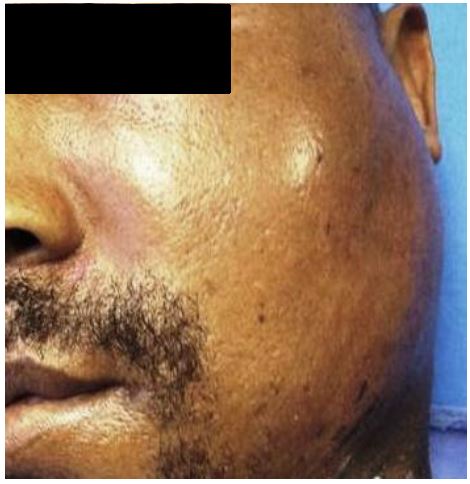
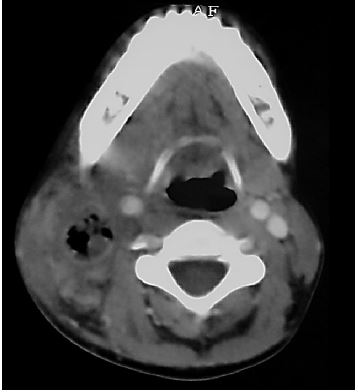
Buccal space sepsis is principally of odon-togenic origin in adults (Figure 15); this includes the maxillary bicuspid and molar teeth and even the mandibular equivalents. However buccal space sepsis in children may have non-odontogenic causes as well. The infection is easily diagnosed as there is often marked cheek swelling, trismus is not severe (Figure 17) and there are often carious bicuspid or molar teeth. More specifically the abscess manifests as loss of the nasolabial skin fold, a rounded, tender cheek swelling, and swelling of the lower eyelid (Figure 17). Diagnostic needle aspiration is easily performed.

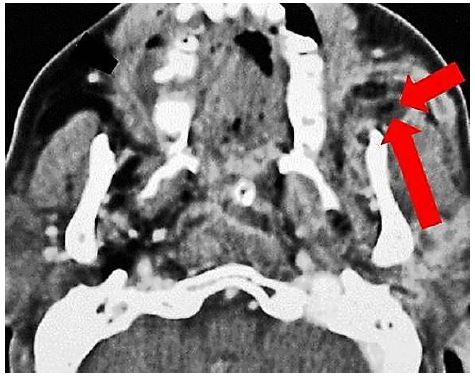
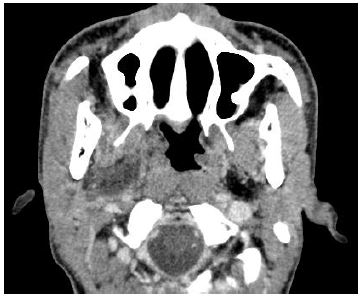
Initial radiology should include an ortho-pantomograph (OPG) or Cone Beam CT (CBCT) to exclude an odontogenic causes. More advanced imaging such as contrast enhanced CT (Figure 18) or MRI may be useful in more complex cases.
Treat the cause, e.g. carious teeth. Trans-oral drainage is done just inferior to the point of fluctuance. Generally an incision is made intra-orally just inferior to the opening of the parotid duct; with necessary care and using blunt dissection only into the periphery of the space, injury to branches the facial nerve is avoided. The intra-oral approach does not allow for dependent drainage.
If one elects to make a more inferiorly placed external incision parallel to the inferior border of the mandible, blunt dissection should be directed superiorly and anteriorly remaining superficial to the masseter. Take care not to injure the marginal mandibular nerve, facial artery or vein.
Alternately one can place incisions in the mandibular and/or maxillary vestibules, and dissect bluntly either inferiorly (mandible) or superiorly (maxilla) through the buccinator muscle into the abscess.
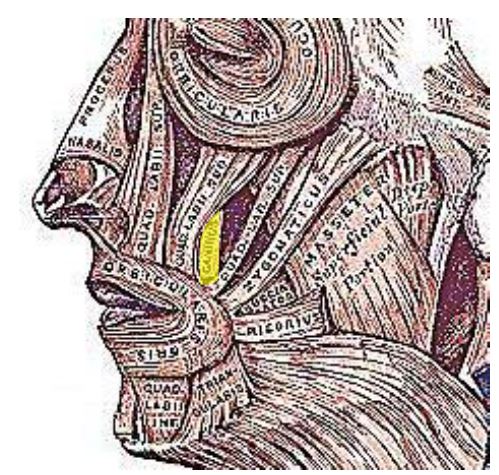
Whether the canine space is a true fascial space or simply a muscular apartment is a matter for debate. A canine space infection is usually caused by maxillary cuspid infection that perforates the lateral cortex of the maxilla above the insertion of the levator anguli oris muscle of the upper lip (Figure 19). The muscle’s origin is the maxillary wall high up in the canine fossa; it inserts into the angle of the mouth with the orbicularis and zygomatic muscles. If infection extends below the insertion of the levator muscle, as is more commonly found, it presents as a swelling of the labial sulcus or, less commonly, as a palatal swelling. However infection of the canine space generally presents as swelling lateral to the nares and of the upper lip (Figure 20). It may cause marked cellulitis of the eyelids (Figure 21) or drain spontaneously, creating a sinus and cause subsequent scarring (Figure 22).

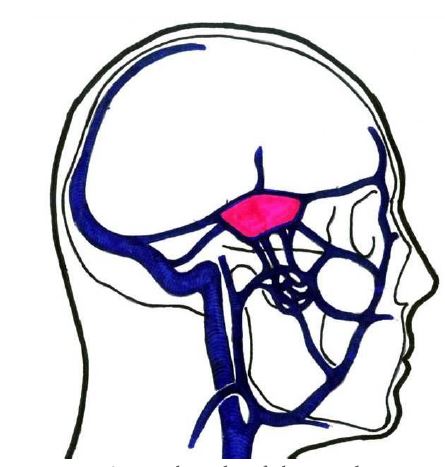
Septic thrombi of the angular vein may extend via the superior and inferior ophthalmic veins to the cavernous sinus and cause cavernous sinus thrombosis with the classical signs of ptosis, proptosis, chemosis and ophthalmoplegia/paresis (Cranial nerves III, IV, VI) (Figure 23).


Drainage is normally achieved via an intra-oral approach, with access high in the maxillary labial vestibule. Dissect superiorly through the levator anguli oris muscle using blunt dissection to avoid injury to the infra-orbital nerve.
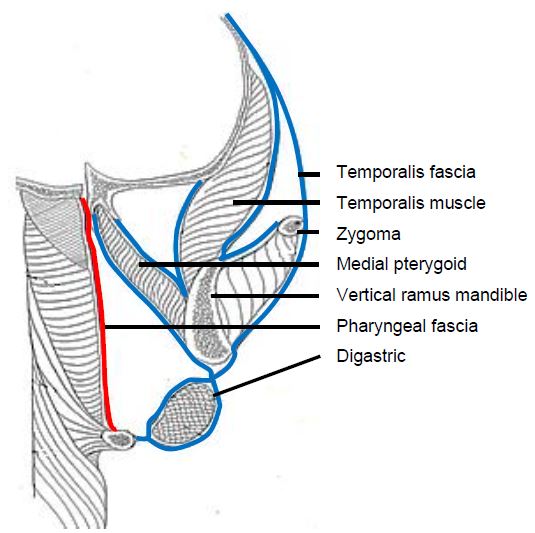
The masticator space(s) is defined by the superficial (investing) layer of deep cervical fascia (Figure 9). It contains the masseter, medial and lateral pterygoids, ramus and body of the mandible, temporalis tendon, and inferior alveolar vessels and nerve. It is related superiorly to the temporal space; posteromedially to the para-pharyngeal space; and posteriorly to the parotid space (Figure 24).
The literature is not consistent about how to define the masticator space and often speaks about “masticator spaces” or a “masticator space with compartments”. The masticator space(s) has masseteric, pterygoid and temporal spaces/compartments which communicate with each other as well as with the buccal, submandibular and parapharyngeal spaces (Figures 25 a, b).
Sepsis is primarily of dental origin, especially from the 3rd inferior molar tooth. Infection may be confined to only one the masticator compartments or may spread to any or all the above mentioned compart-ments/spaces. Patients generally present with local pain and marked trismus. Needle aspiration is a valuable diagnostic tool (Figure 26).

Drainage of abscesses of the masticator spaces will next be discussed according to the individual masseteric, pterygoid and temporal spaces /compartments.
The masseteric (submasseteric) space is located between the masseter muscle laterally and the mandibular ascending ramus medially (Figure 27). Anteriorly, the space is bound by the inner surface of the masseteric fascia and posteriorly by the parotidomasseteric fascia as it splits to envelop the parotid gland. The superior and inferior borders are, respectively, the zygomatic arch and angle and the inferior border of the ramus where the masseter muscle is attached.

Clinically patients present with bulging of the masseter muscle, severe trismus and pain (Figure 28). Due to its submasseteric location, palpation often reveals a non-fluctuant, very firm swelling.

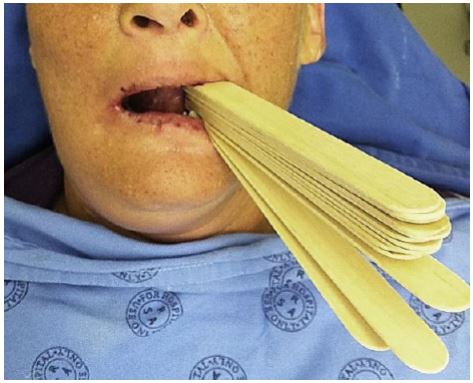
Tongue depressors are a useful aid to overcome the severe trismus and to gain access to the mouth for intra-oral local anaesthetic blocks, incision and drainage procedures and even for intubation (Figure 29).
An external approach is generally employed. An incision is made at the angle of the mandible, parallel to the inferior border of the mandible. After cutting through the skin and subcutaneous tissue, blunt dissect-tion is directed superiorly through the platysma and the submandibular space. Care should be taken to avoid injury to the mandibular branch of the facial nerve. An intra-oral approach can be used via a vertical incision made along the pterygo-mandibular raphe; use blunt dissection lateral to the mandibular ramus and medial/deep to the masseter muscle to reach the abscess. Combined approaches can also be used. Ultrasound-guided drainage can be considered in patients with unilocular submasseteric space infection and severe trismus causing a significant anaesthetic risk.
The pterygoid (pterygomandibular) space consists mostly of loose areolar tissue. It is located between the pterygoid muscles and the ramus of the mandible (Figures 27, 30). Other nomenclature includes “internal pterygoid space” or “superficial pterygoid space”.

It is bound medially and inferiorly by the medial pterygoid muscle and the pterygo-masseteric sling respectively. The lateral pterygoid muscle is located superomedially. The medial ramus of the mandible is located laterally. The parotid gland curves medially around the back of the mandibular ramus to form its posterior border, while anteriorly the buccinator and superior constrictor muscles join to form a fibrous junction, the pterygomandibular raphe. The pterygoid space contains the inferior alveolar nerve, artery and vein, the lingual nerve and the nerve to the mylohyoid muscle.
Sepsis of the pterygoid space is commonly due to infection of the 3rd molar tooth, or results from infection following 3rd molar surgery or mandibular orthognathic surgery; it may also follow mandibular local anaesthetic blocks. Trismus and pain are often the presenting sign and symptom.
An extra-oral submandibular approach is normally employed. Dissect bluntly through the pterygomasseteric sling up to the pterygoid space, remaining medial to the ramus and lateral to the medial pterygoid muscle. An intra-oral approach is done via a vertical incision, lateral and parallel to the pterygomandibular raphe. Blunt dissection is then used to reach the pterygoid space by dissecting along the medial surface of the ramus. A combined approach with through-and-through drains can also be employed.
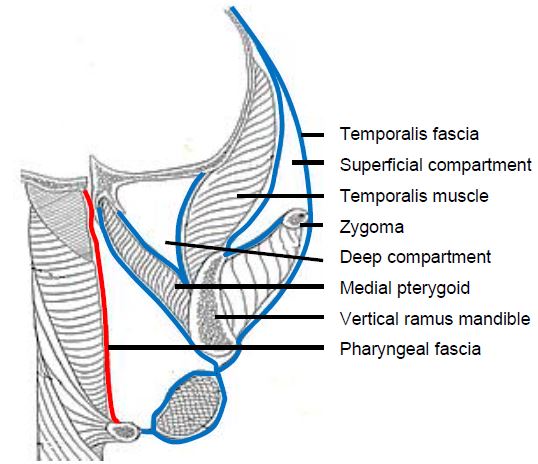
The temporalis muscle partitions this space into deep and superficial compartments. The superficial compartment is contained laterally by the temporalis fascia (superficial/investing layer of deep fascia), and medially by the temporalis muscle; the deep compartment is limited laterally by the deep surface of the temporalis muscle, and medially by the periosteum overlying the temporal bone.
It contains the internal maxillary artery and its branches, the inferior alveolar artery and nerve, and is bisected by the temporalis muscle. It is related inferiorly to the masticator space. Sources of sepsis include maxillary molar infection or post-extraction sepsis; maxillary sinusitis, maxillary sinus fractures; temporomandibular arthroscopy and sepsis following injections into the temporomandibular joint.
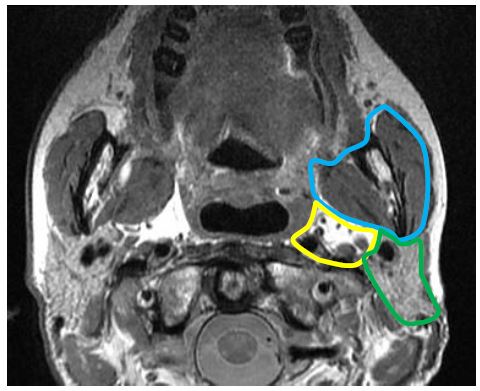
Temporal space sepsis typically presents as swelling of the temporal fossa, pain and trismus. Contrast enhanced CT or MRI scans indicate the relations of the abscess to the temporalis muscle and extension to other spaces e.g. masticator space (Figure 32)
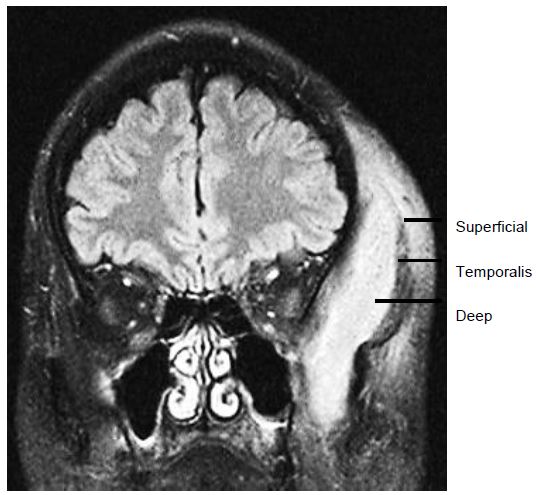
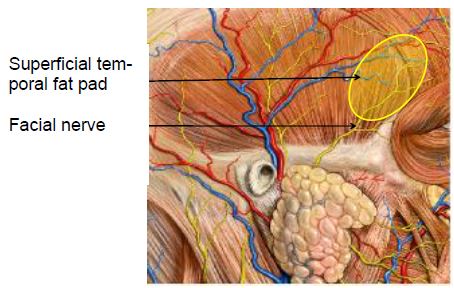
External approach to superficial and deep compartments: An incision is made 3cm lateral to the lateral canthus of the eye taking care not in injure the frontal/ temporal branches of the facial nerve which run across the superficial temporal fat pad, deep to the orbicularis oculi muscle, just lateral to the orbital rim (Figure 33, 34); or by a horizontal brow incision. The deep compartment is drained by advancing a haemostat through the temporalis muscle into the space between the temporalis muscle and temporal and sphenoid bone.

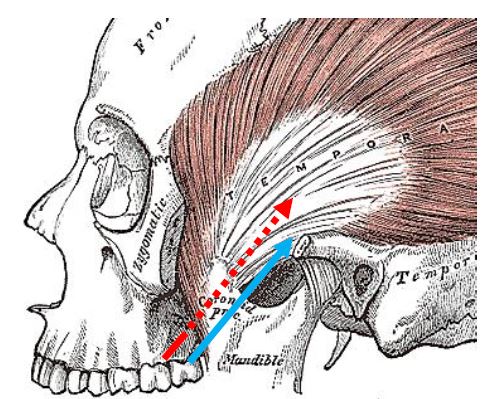
Intra-oral drainage: The temporalis mus-cle attaches to the coronoid process of the mandible (Figure 35). The key anatomical landmark for intraoral drainage therefore is the vertical ramus of the mandible where it ascends from the retromolar trigone. To drain the superficial compartment, make a stab incision in the mucosa lateral to verti-cal ramus of the mandible and advance a haemostat lateral to the coronoid process into the abscess. To drain the deep compartment, make a stab incision in the mucosa medial to the vertical ramus and advance a haemostat medial to the coronoid process into the abscess. A combined approach can also be used.
The parotid space is bound by the superficial (investing) layer of deep cervical fascia (Figures 24, 36). The investing fascia splits at the level of the stylomandibular ligament to enclose the gland by superficial and deep parotid capsules. The space extends from the external auditory canal to the angle of the mandible. It is located lateral to the carotid and parapharyngeal spaces and posterior to the masticator space (Figure 24). It contains the parotid gland, proximal part of the parotid duct, facial nerve, posterior facial/retromandibular vein, intraparotid lymph nodes and terminal branches of external carotid artery. The superficial capsule is strong, but the deep capsule is thin, allowing for infection to spread easily into the para-pharyngeal space.

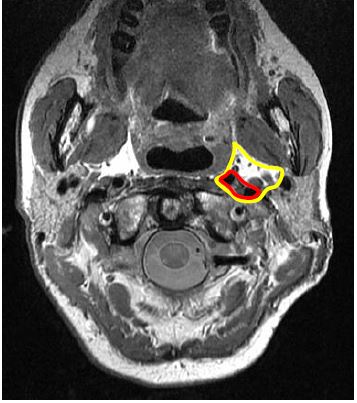
Sources of sepsis include parotitis, sialade-nitis and adjacent sepsis. Parotid space sepsis typically presents with tenderness, swelling, and trismus (Figure 37). Fluctuation is often absent and it may be difficult to distinguish clinically between parotitis and a parotid abscess. Ultrasound or a contrast enhanced CT scan is useful to diagnose a parotid abscess (Figure 36).
Injury to the facial nerve is the principle concern. Incision and drainage is done un-der general anaesthesia by elevating a parotidectomy skin flap to expose the parotid capsule. Incisions are made in the parotid capsule along the axis of the facial nerve, a haemostat is passed bluntly into the abscess(es), and drains are inserted. Resolution of the parotid swelling is generally quite delayed.
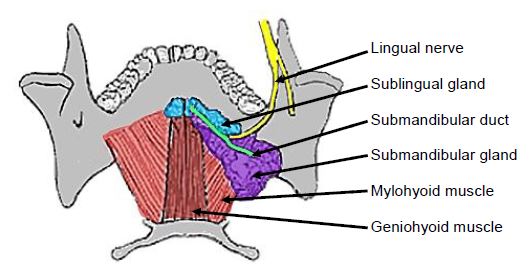
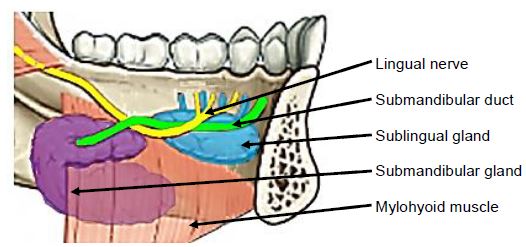
The sublingual space is contained by the mucosa of the floor of the mouth above, the mylohyoid muscle below (Figures 38, 39), and is continuous with the opposite side across the midline. Anteriorly and laterally it is bound by the mandible. The posterior border is the hyoid bone. The space contains the sublingual salivary glands, intra-oral components of the sub-mandibular salivary glands and the sub-mandibular ducts, and the hypoglossal and lingual nerves (Figures 35, 36).
The space is connected with the subman-dibular space at the posterior edge of the mylohyoid muscle around which pus can track; as well as with the submental space inferiorly with mylohyoid muscle inter-posed; and the parapharyngeal space posteriorly.
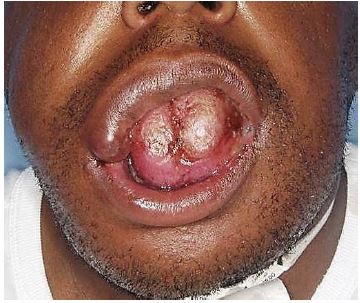
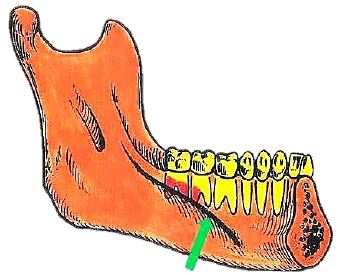
Sources of infection include dental sepsis, especially of the 3rd lower molar tooth, sia-lolithiasis, and an infected ranula. Patients present with pain, swelling, induration in the floor of the mouth and elevation of the tongue (Figure 40-42).
Drain the sublingual space transorally by incising the mucosa in the anterior floor of the mouth, preferably parallel to the submandibular duct, and proceed with blunt dissection taking care not to injure the lingual nerve or the submandibular ducts. If the submandibular space is also affected, both spaces can be reached via a submandibular approach.
The submental space is located below the chin, crosses the midline and is bound superficially by the superficial layer of cervical fascia and skin, laterally by the anterior bellies of the digastric muscles, and deeply by the investing layer of cervical fascia overlying the mylohyoid muscle. The anatomical relations are the sublingual space (above mylohyoid) and the submandibular spaces laterally. It contains fat, lymph nodes and the anterior jugular vein (Figure 43).
Sources of sepsis are typically dental (mandibular incisor), an infected ranula, lymphadenitis or extension of infections of the submandibular space. Patients present with a tender submental swelling (Figures 44, 45).

Drainage is achieved via an external transverse skin incision made between the hyoid bone and the mentum.
A lack of conformity exists in the literature about what is meant by “submandibular space”. Some subdivide the “submandibu-lar space” into submaxillary, sublingual and submental spaces, while others consider the submaxillary and submandibular spaces to be synonymous. To best conform to conventional head and neck surgery terminology, the latter use of the word is adopted in this chapter.
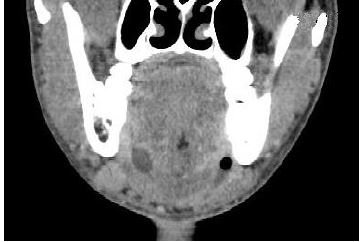
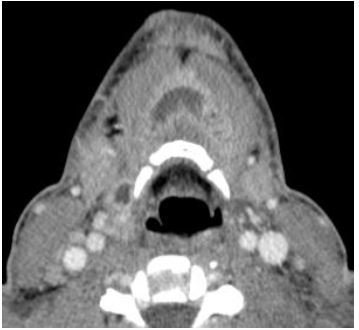
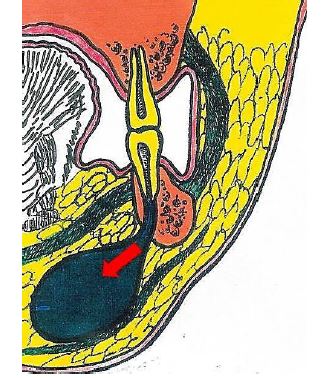
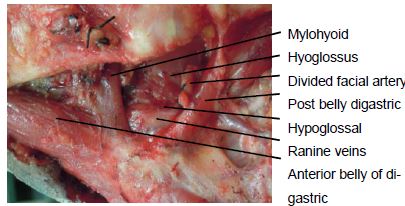
As the most inferior space of the supra-hyoid neck, the submandibular space extends upwards from the hyoid and is contained laterally between the hyoid and mandible by the superficial (investing) layer of deep cervical fascia and by the medial surface of the mandible up to its mylohyoid line (Figures 7, 8, 9, 46). Medially it is limited by the investing fascia that covers the mylohyoid muscle, the hypoglossal nerve, ranine veins and hyoglossus muscle (Figure 47). It contains the superficial portion of the submandibular gland, submandibular and submental lymph nodes, facial artery and vein, fat and the inferior loop of the hypoglossal nerve. The anterior belly of digastric separates it from the submental space (Figure 47). The submandibular gland and its duct pass around the posterior margin of the mylohyoid to enter the sublingual space in the floor of the mouth (Figures 38, 39). Behind the posterior margin of the mylo-hyoid muscle is a direct communication between the submandibular and sublingual spaces. Infection may spread anteriorly to the submental space and posteriorly to the parapharyngeal and/or retropharyngeal spaces.
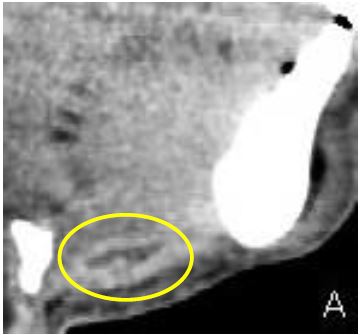
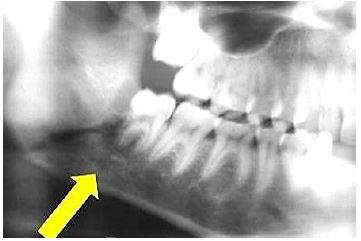
Sources of sepsis include sialoadenitis, sialolithiasis, and dental sepsis (Figures 46, 48, 49). Patients typically present with swelling and tenderness over the submandibular triangle of the neck and only very minor trismus (Figures 50).

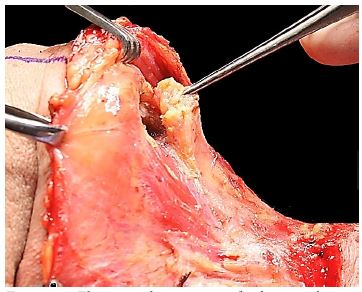
Make a horizontal skin crease incision at the level of the hyoid to avoid transecting the marginal mandibular nerve. Extend the incision through the platysma muscle using blunt dissection (Figures 51, 52).


Ludwig’s Angina, named after Wilhelm Friedrich Von Ludwig (1790-1865) refers to inflammation, cellulitis or an abscess, generally of dental origin, that involves the sublingual, submental and submandibular spaces. “Angina” is derived from the Latin term “angere”, which means “to strangle”. Patients present with pain, drooling, dysphagia, submandibular swelling, trismus. Upward and posterior displacement of the tongue may cause severe airway compromise (Figure 53) which is the primary morbidity and mortality. In the pre-antibiotic era the mortality rate for was 50%; today the mortality rate is <5%. Sepsis is typically bilateral (Figure 54).

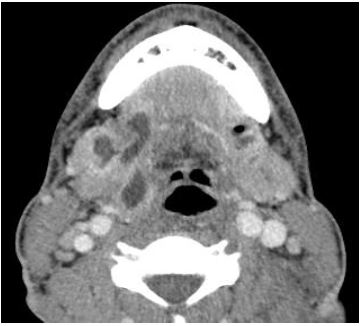
An orthopantomogram (OPG) or a CT scan should be requested to identify the source of dental sepsis; special attention should be paid to the status of the 2nd and 3rd lower molars. A contrast-enhanced CT scan or even MRI provides a roadmap for the surgeon to drain all septic foci in the neck (Figure 54).
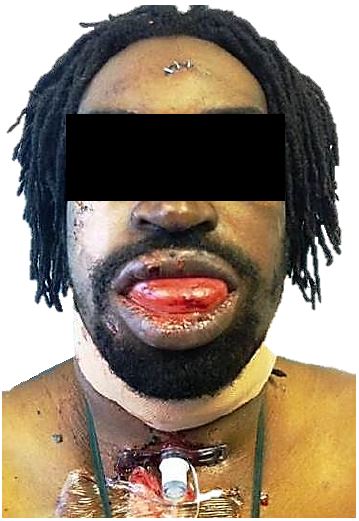
Securing an airway is the initial objective. One should have a low threshold for doing an awake tracheostomy under local anaes-thesia to secure the airway before inducing anaesthesia. Transoral intubation may be hazardous and is often unsuccessful. Fibre-optic intubation requires skill and experience and may cause nasal/nasopharyngeal bleeding (Figure 55).

Nebulised adrenaline (1ml 1:1000 adrena-line diluted to 5ml with 0.9% saline) and intravenous dexamethasone (controversial) has been suggested to create more control-led conditions for flexible nasotracheal intubation. It is important to note that after incision and drainage, there is often even more swelling which may compromise the airway on day 1-2 after the surgery (Figure 56).
Incision and drainage: Ludwig’s angina starts as a rapidly spreading cellulitis without lymphatic involvement and generally without abscess formation. There is absolute consensus that drainage is indicated when there is a suppurative infection and/ or radiological evidence of a fluid collection or air in the soft tissues.
However one of the main controversies in management of Ludwig’s angina is whether surgical drainage is always indicated in the earlier stages of the infection. In the authors’ experience, a more aggressive surgical approach should be followed in all cases i.e. early tracheostomy and empiric placement of drains in the affected spaces after removal of the underlying cause. It must however be noted that this combined medical and surgical protocol is dictated by surgical/anaesthesia/intensive care logistical problems often experienced in developing world practice.
Drainage may be intraoral and/or external, depending on the spaces involved. The submandibular spaces are drained externally. If sepsis extends both above and below the mylohyoid muscle, through-and-through drains extending between the oral cavity and the skin of the neck may be inserted.
The PPS extends from the base of the skull to the hyoid bone as an inverted pyramid in the centre the head and neck, and consists mostly of fat. It is also known as the lateral pharyngeal space, pterygomaxillary space or pharyngomaxillary space.
Medially it is defined by the visceral layer of the deep cervical fascia (pharyngo-basilar fascia above and buccopharyngeal fascia covering the superior pharyngeal constrictor muscle). The posterior border is formed by the prevertebral fascia of the deep layer and by the posterior aspect of the carotid sheath. Laterally the space is limited by the superficial/investing layer of deep cervical fascia that overlies mandible, medial pterygoids and parotid. The anterior boundary is the interpterygoid fascia and the pterygomandibular raphe.
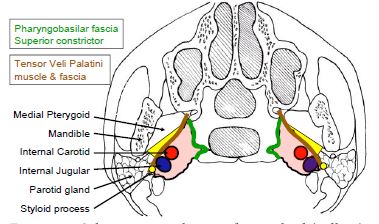
The space is often divided into a prestyloid and a poststyloid compartment/space as the styloid process and styloid fascia divides this space. Some authors elect to use the terms prestyloid parapharyngeal space and parapharyngeal space synonymously as the poststyloid parapharyngeal space is regarded as a separate space namely the carotid sheath or space. Figure 57 illustrates the prestyloid and poststyloid components of the PPS, separated by the styloid process, tensor veli palatini and its fascia. The prestyloid PPS contains the internal maxillary artery, inferior alveolar nerve, lingual nerve, and auriculotemporal nerve, the deep lobe of the parotid gland, fat and occasionally ectopic salivary gland tissue. The poststyloid space encompasses the carotid space and contains the internal carotid artery, internal jugular vein, cranial nerves IX - XII, and the sympathetic trunk (Figure 57).
The PPS (Figure 58) is a central connection for all other deep neck spaces and was the most commonly affected space before the modern antibiotic era. It interfaces posterolaterally with the parotid space, posteromedially with the retropharyngeal space and inferiorly with the sub-mandibular space. Anterolaterally it abuts the masticator space. The carotid space courses through the PPS. Infections can arise from tonsils, pharynx, teeth, salivary glands, nose, or may extend from a Bezold’s abscess (mastoid abscess).
Medial displacement of the lateral pharyn-geal wall and tonsil is a hallmark of PPS infection (Figures 59-62). Trismus, drooling, dysphagia, odynophagia, neck stiffness, a “hot potato” voice and swelling below the angle of the mandible may be present when the anterior compartment is involved. The ipsilateral neck pain can be intensified by lateral flexion of the neck to the contralateral side which compresses the lateral pharyngeal space. Trismus suggests inflammation of the pterygoid muscle which lies close to the anterior compartment. Infection of the posterior compartment often has no trismus or visible swelling.
Three approaches may be employed de-pending on the location of the abscess. Additional approaches may be considered to drain adjacent sepsis.
The prestyloid PPS may be drained trans-orally (Figure 61) by incising the lateral pharyngeal wall, or via a suprahyoid approach (Figure 62).
The retrostyloid PPS is best approached transcervically from Level 2a of the neck. A transverse cervical skin incision is made, and subplatysmal flaps elevated to expose the anterior border of sternomastoid. The investing layer of deep cervical fascia is divided along the anterior border of the sternocleidomastoid, and a finger is passed deep to the posterior belly of digastric, dissecting bluntly along the carotid sheath up to the tip of the styloid.
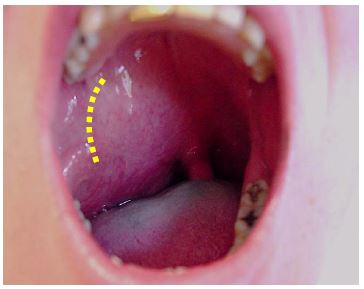
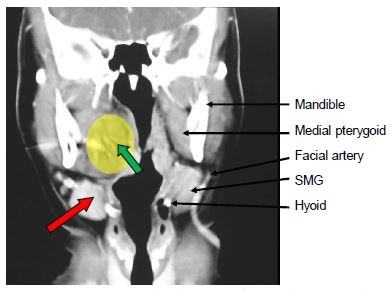
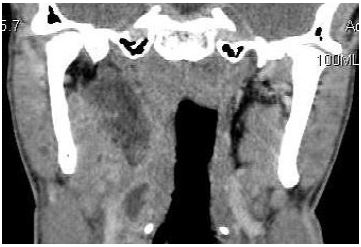
The peritonsillar space is bound medially by the capsule of the palatine tonsil, laterally by the superior constrictor, while the anterior and posterior borders are defined by the anterior and posterior tonsillar pillars. It is a potential space and has no important contents, mostly loose connective tissue. Laterally it abuts the masticator space; this accounts for the typical occurrence of trismus with inflammatory pro-cesses. Posteriorly it borders the parapharyngeal space.
Peritonsillar abscesses (Figure 63) are the most common deep neck space abscesses and occur as a consequence of tonsil infection. It has also been proposed that it is a consequence of inflammation of Weber’s glands which are minor salivary glands found in the peritonsillar space.
Patients typically present with pain, odyno-phagia, drooling, dehydration, trismus, medial displacement of the tonsil, palatal asymmetry, oedema and contralateral dis-placement of the uvula (Figure 64). The diagnosis is clinical and special radiological investigations are usually unnecessary.

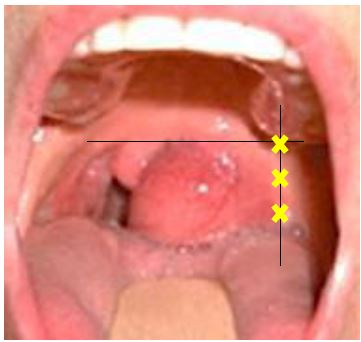
Peritonsillar abscesses may be treated by needle aspiration, incision and drainage, or quinsy tonsillectomy.
Needle aspiration/Incision and drainage: Local anaesthetic is injected along the anterior tonsillar pillar followed by transoral needle aspiration and/or incision and drainage with a scalpel superomedially. The incision is then opened widely with a haemo-stat. The classical needle aspiration sites are demonstrated in Figure 64. A needle inserted too medially will enter the tonsil tissue and miss the abscess cavity.
Quinsy tonsillectomy: This is advocated by some surgeons for patients with recurrent tonsillitis or in children who would not tolerate a procedure under local anaesthesia. The patient, however, should first be rehydrated and optimised for surgery. As trismus is generally due to muscle spasm, it resolves on induction of anaesthesia. Hence intubation is generally not a problem. The tonsillectomy on the side of the quinsy is usually quite straight-forward once the abscess cavity has been entered as the abscess wall defines the lateral dissection plane. Bipolar cautery is required for haemostasis as ligating vessels in inflamed tissues may prove difficult.
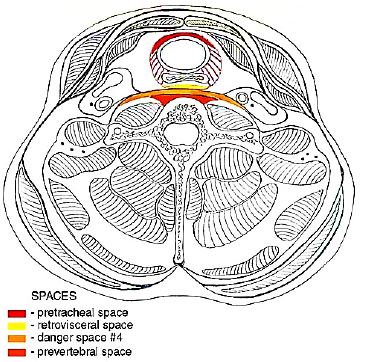
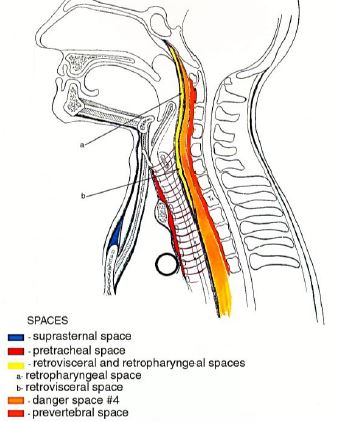
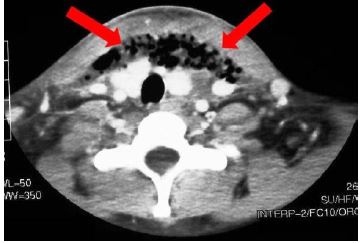
The pretracheal (anterior visceral or pre-visceral space) is enclosed by the visceral layer of the middle layer of deep cervical fascia. It lies immediately anterior to the trachea, abuts the ventral wall of the oeso-phagus posteriorly and extends from the superior border of the thyroid cartilage to the superior mediastinum at level T4 (Figures 65 a, b). Aetiology includes perforation of the anterior oesophageal wall by endoscopic instrumentation, foreign bodies, trauma and thyroiditis. Patients present with dysphagia, odynophagia, pain, fever, voice change and stridor.
Drainage is achieved by a transverse anterior skin crease cervical incision.
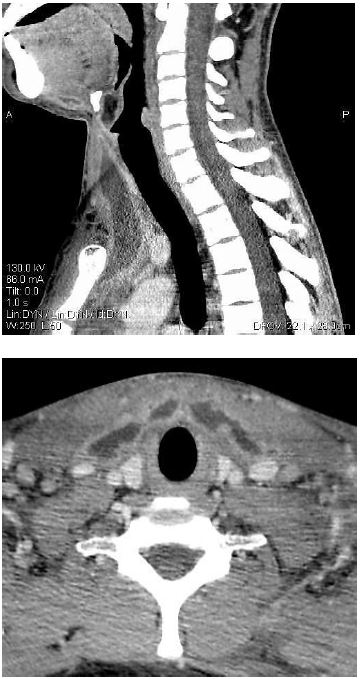
The retropharyngeal space is located immediately behind the nasopharynx, oro-pharynx, hypopharynx, larynx, and trachea. It is bound anteriorly by the visceral layer of the middle layer of the deep cervical fascia where it surrounds the pharyngeal constrictors, and posteriorly by the alar layer of the deep layer of deep cervical fascia. It extends from the skull base to T2/tracheal bifurcation where the visceral and alar layers fuse (Figures 2, 3, 4). It contains retropharyngeal lymphatics and lymph nodes, and communicates laterally with the parapharyngeal spaces where it abuts the carotid sheaths.
Because retropharyngeal lymph nodes generally regress by age 5yrs, retro-pharyngeal space infection occurs more commonly in young children. Most retro-pharyngeal abscesses in children are related to upper respiratory tract infections. In adults they are generally caused by direct trauma and foreign bodies, and may also be caused by traumatic perforations of the posterior pharyngeal wall or oesophagus. Sepsis may also extend from the para-pharyngeal space, or from infections originating in the nose, adenoids, naso-pharynx, and sinuses. The differential diagnosis includes an abscess secondary to spinal tuberculosis.
Patients present with malaise, neck stiffness, odynophagia, bulging of the posterior pharyngeal wall, trismus, stertor or stridor. Sepsis may extend posteriorly to the prevertebral space, into the chest causing mediastinitis and empyema, or laterally to the parapharyngeal space. It can cause carotid artery rupture and jugular vein thrombosis. CT is the imaging investigation of choice. Lateral cervical X-rays show loss of cervical lordosis and widening of the prevertebral soft tissues which should normally be less than ½ the width of the corresponding vertebral body (Figure 66). CXR or CT is done to exclude intrathoracic extension of sepsis.

Sedation and muscle relaxants should be avoided to prevent loss of control of the airway.
Small abscesses may be aspirated trans-orally with a needle in a compliant patient. Larger abscesses require incision and drainage using transoral and/or transcervical approaches.
With transoral drainage it may be helpful to localise the abscess by first aspirating it before incision and drainage. Make an incision through the posterior pharyngeal wall mucosa, and open the abscess with blunt dissection.
Transcervical drainage is achieved by a transverse cervical skin incision, raising subplatysmal flaps to expose the neck and dissecting along the anterior border of the sternomastoid. The sternocleidomastoid muscle and carotid sheath are then retrac-ted laterally and blunt dissection is done up to the hypopharynx to open the retro-pharyngeal space abscess.
The term “danger space” is derived from the potential for rapid spread of infection along this space to the posterior mediastinum. It is a potential space that contains mostly fat. It is located between the alar and prevertebral layers of the deep layer of deep cervical fascia and laterally is bordered by the transverse processes (Figure 67, 68). It is immediately posterior to the retropharyngeal space, anterior to the prevertebral space, and extends from the skull base above to the posterior mediastinum and diaphragm below.
http://cosmos.phy.tufts.edu/~rwillson/dentgross/headneck/Index.htm
http://cosmos.phy.tufts.edu/~rwillson/dentgross/headneck/Index.htm
Infection usually originates from adjacent retropharyngeal, parapharyngeal, or pre-vertebral sepsis and may spread rapidly because of the loose areolar tissue that occupies this space to cause mediastinitis (Figure 69), empyema, and septicaemia.
Clinically the infection is difficult to distinguish from infection of the retropharyn-geal space. Even contrast-enhanced CT may not adequately differentiate between infection of the retropharyngeal and danger spaces, but extension below T4 suggests involvement of the danger space. The differential diagnosis includes tuberculosis.
Surgical drainage is achieved by an external transcervical approach along the anterior border of the sternocleidomastoid, dissecting between the larynx and the carotid sheath. One may need to divide the superior thyroid artery for access.
The carotid space is a potential space contained within the carotid sheath (Figure 70). The nomenclature is confusing and terms such as carotid sheath and post-styloid parapharyngeal space (PPS) are used synonymously. The carotid sheath is formed by the muscular layer of the middle layer of deep cervical fascia. The investing layer of deep cervical fascia contributes to the anterior wall (Figures 3, 4).
The space contains the internal carotid artery, internal jugular vein, cranial nerves IX-XII, lymph nodes and the sympathetic trunk. Above the level of the hyoid bone it is contained within the retrostyloid com-ponent of the PPS (Figure 71). In the suprahyoid neck the space is bordered anteriorly by the styloid process and the PPS, laterally by the anterior belly of digastric and the parotid space and medially by the lateral margin of the retropharyngeal space.
Sepsis may originate from infection within the PPS, from intravenous drug abuse, central venous (CVP) line sepsis, or from lateral sinus thrombosis related to mastoiditis (Figure 71). Patients may initially not have localising signs as the infection is deep-seated. Often clinical signs may only become evident after onset of neurological or vascular complications. Patients may present with torticollis to the side opposite to the sepsis, and tenderness along the course of the carotid. They lack trismus. Vascular complications include suppurative jugular vein thrombophlebitis (Lemierre syndrome), septic pulmonary emboli, carotid artery thrombosis, carotid aneurysm, stroke, or carotid or jugular vein blowouts. Involvement of the sympathetic trunk can cause Horner’s syndrome. Contrast enhanced CT is recommended. Duplex ultrasonography can identify vascular complications.
Treatment is directed at drainage of the sepsis via a transverse cervical skin crease incision with elevation of subplatysmal flaps superiorly and inferiorly for exposure. Clot propagation and pulmonary emboli are limited by anticoagulation.
This is a potential space and extends from the skull base to the coccyx. Due to the anatomy of the potential space, it has also been named the perivertebral space. It is divided into two divisions, namely the prevertebral and paraspinal spaces. It is immediately posterior to the Danger Space and is bound anterolaterally by the carotid space. It is located anterior to the vertebral bodies, behind the prevertebral fascial layer of the deep layer of deep cervical fascia that separates it from the Danger Space (Figures 67, 68). Laterally it is limited by the fusion of the prevertebral fascia with the transverse processes of the vertebral bodies.
Infection may be caused by trauma, especially surgery, or may originate from the cervical or thoracic spine. The diagnosis is difficult to make. Patients may present with neck and/or back pain, just fever and/or neurologic dysfunction ranging from nerve root pain to paralysis. MRI is the imaging modality of choice to assess epidural or spinal cord involvement.
Incision and drainage may be done using transoral or transcervical approaches. The latter approach is made along the anterior border of sternocleidomastoid, dissecting between the larynx and the carotid sheath. One may have to divide the superior thyroid artery for access.
Antibiotics should initially be administered empirically, parenterally, at high doses, and should cover a broad spectrum of oral flora i.e. gram-positive, gram-negative, and anaerobic organisms. The literature advises empiric treatment with combinations of penicillin, clindamycin, and metronidazo-le. The authors favour a combination of penicillin G and metronidazole. Alternatively, amoxicillin-clavulanate with metroni-dazole can be used, or clindamycin for patients who are allergic to penicillin. Antibiotic cover needs to be extended to cover Methicillin-resistant Staphylococcus aureus (MRSA) and gram-negative rods in immune compromised patients. Antibiotics should be modified based on the results of microscopy, culture and sensitivity reports.
http://cosmos.phy.tufts.edu/~rwillson/dentgross/headneck/Index.htm
Jean Morkel BChD, MBChB, MChD, FCMFOS
Professor and Academic Head
Department of Maxillo-Facial and Oral Surgery and Anaesthesiology & Sedation
Faculty of Dentistry
University of the Western Cape
Cape Town
South Africa
jamorkel@uwc.ac.za
Johan Fagan MBChB, FCORL, MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town
South Africa
johannes.fagan@uct.ac.za