The facial nerve is central to parotid surgery for both surgeon
and patient. Knowledge of the surgical anatomy and the landmarks to
find the facial nerve are the key to preserving facial nerve function.
Surgical Anatomy
Parotid gland
The parotid glands are situated anteriorly and inferiorly to the
ear. They overlie the vertical mandibular rami and masseter muscles,
behind which they extend into the retromandibular sulci. The glands
extend superiorly from the zygomatic arches and inferiorly to below the
angles of the mandible where they overlie the posterior bellies of the
digastric and the sternocleidomastoid muscles. The parotid duct exits
the gland anteriorly, crosses the masseter muscle, curves medially
around its anterior margin, pierces the buccinator muscle, and enters
the mouth opposite the 2nd upper molar tooth.
Superficial Muscular Aponeurotic System and Parotid Fascia
The Superficial Muscular
Aponeurotic
System (SMAS) is a fibrous network that invests the facial
muscles, and
connects them with the dermis. It is continuous with the platysma
inferiorly;
superiorly it attaches to the zygomatic arch. In the lower face, the
facial
nerve courses deep to the SMAS and the platysma. The parotid glands are
contained within two layers of parotid fascia, which extend from the zygoma above and continue as
cervical
fascia below.
Structures that traverse,
or are found within the parotid gland
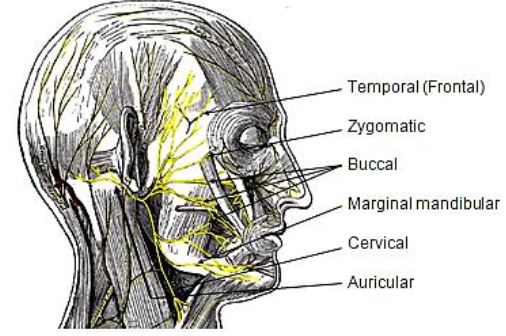
Facial nerve and branches(Figure
1)
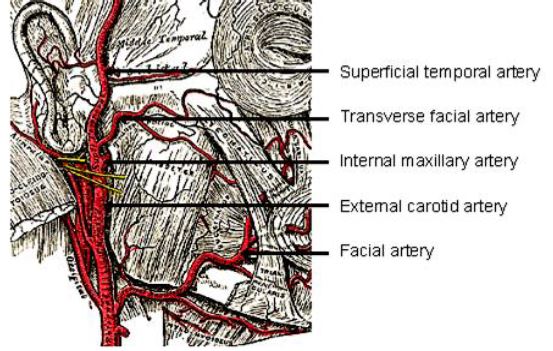
External carotid artery: It gives off
the transverse facial arteryinside the
gland before dividing into the internal maxillary and the superficial
temporal arteries (Figure 2)
Figure 1: Main branches of
facial nerveFigure 2: Branches of external
carotid artery
Veins: The maxillary
and superficial temporal veins merge into
the retro-mandibular vein within the parotid gland, but are not
responsible for draining the gland. Venous drainage of the parotid
itself is to tributaries of external and internal jugular veins.
Lymphatics: A number of lymph nodes are
present within the gland, principally in the superficial lobe, and
drain to Level 2 of the neck.
The facial nerve exits the stylomastoid foramen, and enters the
parotid gland. Although the branching pattern does vary from patient to
patient, the trunk generally divides at the pes anserinus
into upper and lower divisions that subsequently branch into temporal
(frontal), zygomatic, buccal, marginal mandibular and cervical branches
that innervate the muscles of facial expression. Small branches to the
posterior belly of digastric, stylohyoid, and auricular muscles also
arise from the trunk (Figure 3).
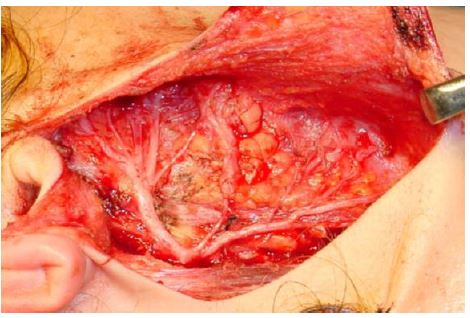
Figure 3: The facial nerve
trunk dividing
into superior and inferior divisions at the pes anserinus
The nerve traverses the parotid gland, with about 2/3 of the gland
substance being superficial to the nerve. As parotid dissection
generally is directed along the facial nerve, the nerve in effect
divides the parotid from a surgical perspective into superficial and
deep lobes, although there is no natural soft tissue dissection plane
that separates the two lobes.
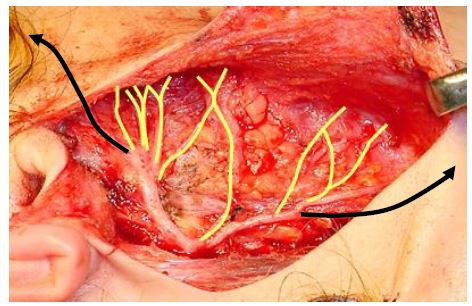
The midfacial nerve branches have multiple cross-innervations;
however the frontal and marginal mandibular branches do not have
cross-innervations and injury to these branches is followed by
paralysis of the forehead and depressors of the lower lip (Figure
4). Therefore unlike the temporal and marginal mandibular nerves,
selected midfacial branches may be sacrificed without loss of facial
function.
Figure 4: Midfacial branches
(yellow)
interconnect whereas temporal and marginal mandibular (black) do not
Locating the Facial Nerve
It is useful to know preoperatively whether a parotid tumour is
situated deep or superficial to the facial nerve. This facilitates
surgical planning and facilitates preoperative consent relating to the
likelihood of a temporary postoperative facial nerve weakness.
Surface markings
Facial nerve trunk: The trunk exits the
skull at the stylomastoid foramen. This is situated at the deep end of
the tympanomastoid suture line, which can be located at the junction
between the mastoid process and the tympanic ring of the external ear
canal
Temporal (frontal) branch of facial nerve:
The nerve crosses the zygomatic arch; it runs within the SMAS and lies
superficial to the deep temporalis fascia. It courses more or less
along a line drawn between the attachment of the lobule of the ear to a
point 1.5 cm above the lateral aspect of the eyebrow. To avoid injury
to the temporal branch dissect either in a subcutaneous plane or deep
to the SMAS (Figure 1).
Radiology
Radiological investigation is not routinely required with parotid
tumours. It is recommended for surgical planning with tumours that are
large, fixed, and are associated with facial nerve involvement,
trismus, and parapharyngeal space involvement. MRI is a valuable
investigation with recurrence of pleomorphic adenoma as it is often
multifocal.
The extratemporal facial nerve is not visible with ultrasound, CT or
MRI. The retromandibular vein is however intimately associated with the
facial nerve. The vein courses through the parotid gland immediately
deep to the facial nerve, but rarely runs immediately superficial to
the nerve (Figures 5 & 6). Reliance is therefore placed
on the juxtaposition of the retro-mandibular vein and the nerve to
predict whether a tumour is likely to be deep or superficial to the
nerve.
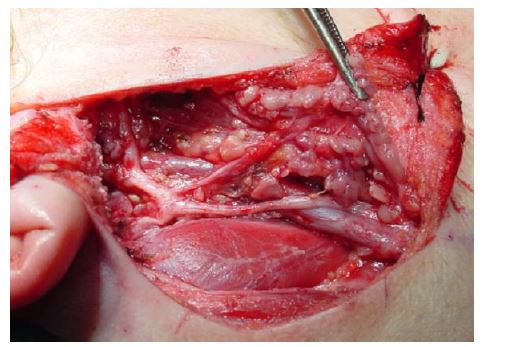
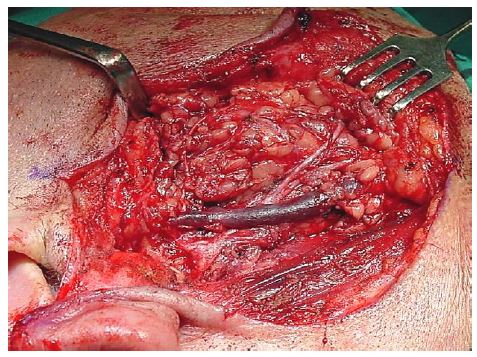
Figure 5: Facial nerve running
superficial to
retromandibular veinFigure 6: Facial nerve running
deep,
but
close, to retromandibular vein
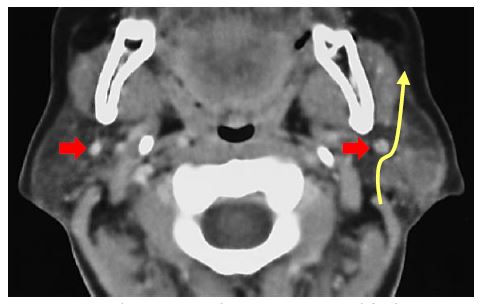
The retromandibular vein can be clearly visualized on a CT with
contrast, or an MRI (Figures 7, 8).
Figure 7: Red arrows indicate
retromandibular
veins, and yellow arrow the course of the facial nerve in a superficial
lobe pleomorphic adenoma
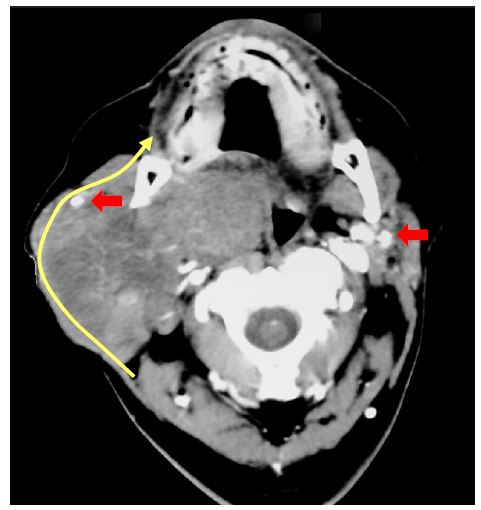
Figure 8: Red arrows indicate
retro-mandibular veins, and yellow
arrow the course of the facial nerve in a deep lobe pleomorphic adenoma
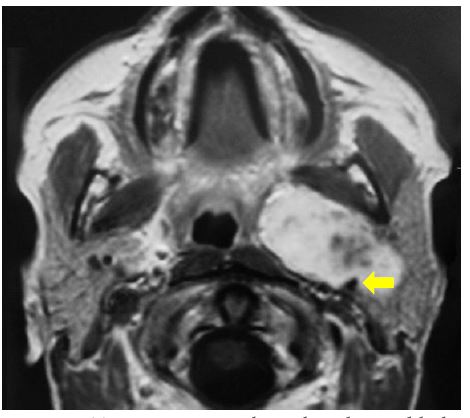
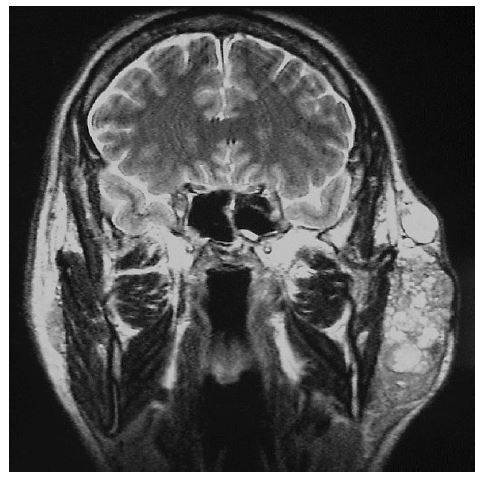
Radiology may also alert the surgeon to extension of a deep lobe
parotid tumour through the stylomandibular tunnel into the
parapharyngeal space (Figure 9).
Figure 9: Tumour passing
through
stylomandibular tunnel to parapharyngeal space (Arrow indicates styloid
process)
Intraoperative location of facial nerve
The facial nerve is usually explored by prograde dissection i.e.
by locating the nerve trunk where it exits from the stylomastoid
foramen, and then dissecting anteriorly along the trunk, the pes
anserinus and the divisions and nerve branches. Occasionally this
is not possible e.g. with a large fixed mass centered at the
stylomastoid foramen. In such cases a retro-grade dissection may be
required after locating the temporal branch where it crosses the
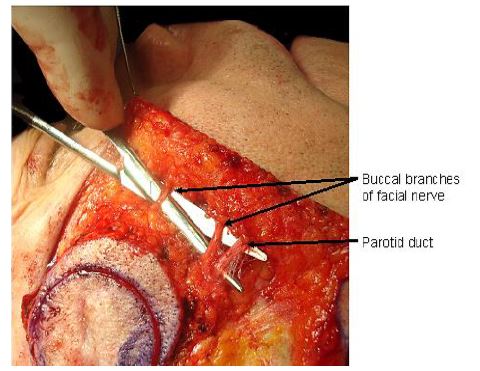
zygoma, the buccal branches which lie parallel to the parotid duct (Figure
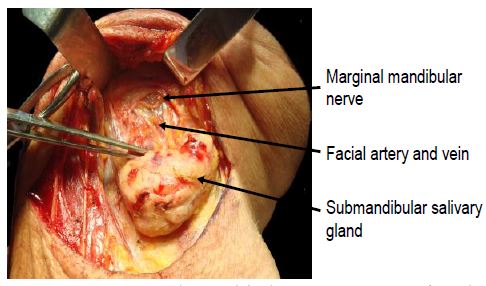
10), or the marginal mandibular branch where is crosses the facial
artery and vein just below or at the inferior margin of the mandible,
where it is just deep to platysma (Figure 11).
Figure 10: Buccal branches
adjacent to the
parotid ductFigure 11: Marginal
mandibular nerve crossing facial artery and vein
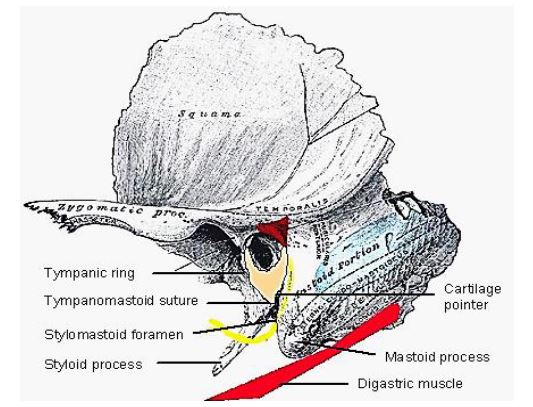
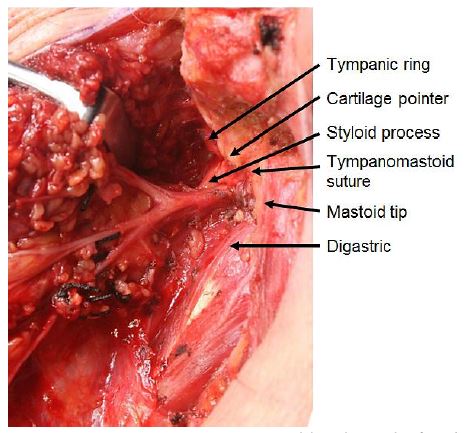
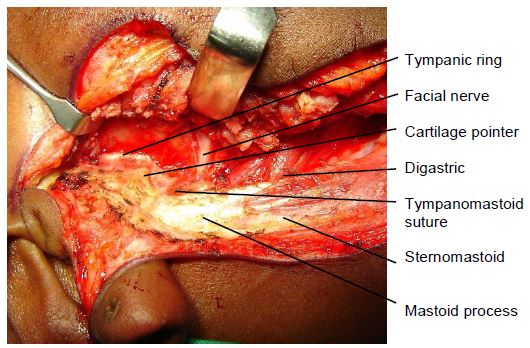
The surgical landmarks for finding the facial nerve trunk at the
stylomastoid fora-men are remarkably constant, and all the landmarks
should be identified at every operation to facilitate finding the nerve
(Figures 12, 13).
Figure 12: Schematic surgical
landmarks for
the facial nerve trunkFigure 13: Intraoperative
surgical land-marks
for the facial nerve trunk
Posterior belly of digastric muscle: The
nerve runs at the same depth below the skin surface, and bisects the
angle between the muscle and the styloid process
Cartilage pointer: This refers to the
medial-most, pointed end of the cartilage of the external auditory
meatus. The nerve exits the foramen approximately 1cm deep and 1cm
inferior to this point
Tympanic ring, mastoid process and tympanomastoid suture
line: The tympanomastoid suture line is the most precise
landmark for the facial nerve as it leads medially, directly to the
stylomastoid foramen
Styloid process: The facial nerve crosses
the styloid process. Palpating the styloid process is therefore a
useful means to determine the depth and position of the facial nerve
Branch of occipital artery: A small branch
of the occipital artery is commonly encountered just lateral to the
facial nerve close to the stylomastoid foramen. Brisk arterial bleeding
should therefore alert the surgeon to the proximity of the facial
nerve; it is easily controlled with bipolar cautery.
Electrical stimulation and monitoring
These need not be routinely employed, but may be useful adjuncts to
a sound know-ledge of facial nerve anatomy in selected cases such as
revision surgery and with large tumours. It may however not record
facial stimulation with faulty equipment, and nerve fatigue following
excessive mechanical or electrical stimulation, and use of a muscle
relaxant.
Electrophysiological monitoring:An EMG monitor may be used to detect contraction of the
facial muscles when the facial nerve is mechanically or electrically
stimulated.
Facial nerve electrical stimulation:Battery operated or more sophisticated nerve stimulators
may be employed intraoperatively to assist with finding the nerve, or
to differentiate between nerve and blood vessels. Stimulating the nerve
produces visible contraction of the facial musculature or an EMG signal.
Types of Parotidectomy
Partial parotidectomy: Resection of
parotid pathology with a margin of nor-mal parotid tissue. This is the
standard operation for benign pathology and favourable malignancies
Superficial parotidectomy: Resection of
the entire superficial lobe of parotid (Figure 3) and is
generally used for metastases to parotid lymph nodes e.g. from skin
cancers, and for high grade malignant parotid tumours.
Total parotidectomy: This involves
resection of the entire parotid gland, usually with preservation of the
facial nerve
Preoperative consent
Scar: Usually very good healing except
over the mastoid where some scarring may occur
Anaesthesia in the greater auricular distribution:
Skin of inferior part of auricle, and overlying the angle of the
mandible
Facial nerve weakness: Temporary
weakness common (<50%); permanent weakness rare
Facial contour: loss of parotid tissue
leads to a more defined angle of mandible, and deepening of
retromandibular sulcus
Prominence of auricle: This is probably
due to loss of innervation of the postauricular muscles and
preauricular scarring
Frey’s syndrome (gustatory sweating):
Although common, it only very rarely is bad enough to require treatment
with Botox injection
Anaesthesia
General anaesthesia
Short-acting muscle relaxation for intubation only, so that
facial nerve may be stimulated and/or monitored
No perioperative antibiotics unless specifically indicated
Hyperextend the head, and turn to opposite side
Infiltrate with vasoconstrictor along planned skin incision, so
as to reduce thermal injury to skin from electro-cautery to skin vessels
Keep corner of eye and mouth exposed so as to be able to see
facial movement when facial nerve mechanically or electrically
stimulated (Figure 14)
Partial/Superficial Parotidectomy
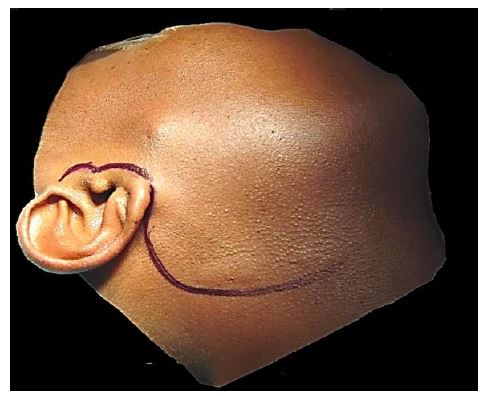
Lazy-S incision: This is placed in pre-auricular and cervical
skin creases (Figure 14)
Figure 14: "Lazy-S”
incision; Corners of eye and mouth exposed
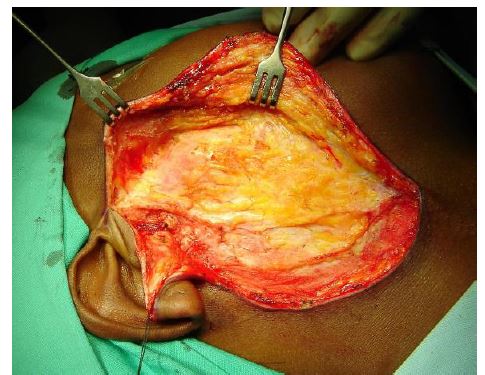
Raise superficial cervicofacial flap to the anterior border of
parotid mass or of the parotid gland in the plane between the SMAS and
the parotid fascia with a scalpel or diathermy. The assistant must
monitor the face for muscle contraction to avoid facial nerve injury.
Insert a traction suture in the subcutaneous tissue of the ear lobule
as well as securing the anterior based skin flap to the drapes (Figure
15)
Figure 15: Exposure of parotid
mass or gland
Skeletonise the anterior border of sternocleidomastoid muscle (Figure
16)
Divide the external jugular vein
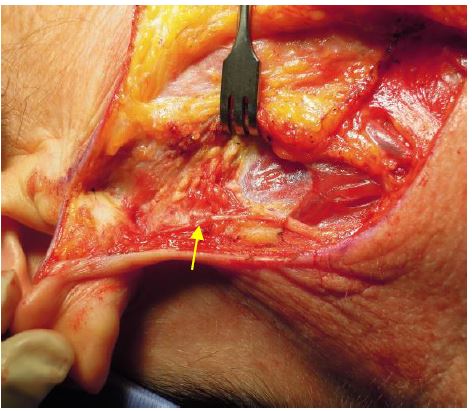
Divide the greater auricular nerve as it crosses
sternocleidomastoid muscle, posterior to the external jugular vein. An
attempt can be made to preserve the posterior branch of the nerve to
retain sensation of the skin of the auricle (Figure 17)
Figure 16: Expose the
sternomastoid and
posterior belly of digastric muscleFigure 17: Posterior branch of
greater
auricular nerve (arrow)
Identify and skeletonise the posterior belly of the digastric
muscle. Do not dissect cephalad of the muscle as one may injure the
facial nerve (Figure 16)
Skeletonise the cartilage of the external auditory canal up to
the tragal pointer. This can be done quite quickly with electrocautery
dissection as the facial nerve exits the stylomastoid foramen 1cm deep
to the tragal pointer
Skeletonise the mastoid tip to the depth of the tragal pointer
Identify all the following landmarks for the facial nerve (Figures
12, 13 & 18)
Tragal pointer (nerve 1 cm deep and inferior)
Tympanic ring
Anterior aspect of mastoid bone
Tympanomastoid suture line (leads directly to stylomastoid
foramen)
Posterior belly of digastric muscle (Facial nerve at same
depth, just above muscle)
Palpate the styloid process (facial nerve in angle between
styloid and digastric, and crosses styloid more anteriorly)
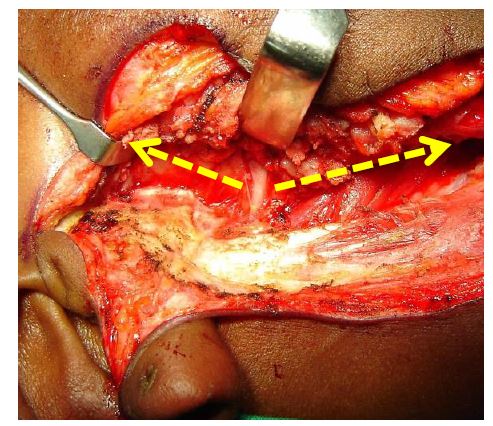
Locate the facial nerve trunk by blunt dissection with a fine
haemostat (Figures 18, 19)
Figure 18: Identify facial
nerve landmarksFigure 19: Location of facial
nerve
trunk,
and superior and inferior release of capsule and parotid tissues
(yellow arrows)
Use fine curved blunt tipped scissors for the remainder of the
nerve dissection Tunnel and spread the tissues overlying the facial
nerve and its branches, and divide the parotid tissue overlying the
nerve. It is important to dissect directly on the nerve so as not to
lose sight of it. Never
divide parotid tissue beyond exposed facial nerve. Wearing loupes e.g.
with 2.5x magnification assists with the dissection, and enables one to
better distinguish be-tween blood vessels and nerves. Employ bipolar
diathermy and fine silk ties for haemostasis.
Dissect along the trunk to the pes anserinus
Dissect back towards the stylomastoid foramen to exclude early
branching from the trunk
Divide the parotid fascia and parotid tissue superiorly and
inferiorly to release the parotid posteriorly and to permit anterior
mobilisation of the gland/tumour (Figure 19)
Dissect along, and strip the superficial lobe off the branches of
facial nerve. Unless a complete superficial parotidectomy is done, only
the branches close to the mass are dissected and exposed (Figure
20)
Figure 20: Strip the
superficial lobe off the
branches of facial nerve
Identify the retromandibular vein as it crosses the medial to the
facial nerve (Figure 21)
If removing the superior part of the gland, identify/ligate the
superficial temporal artery superiorly, just anterior to auricle
If dissecting to the anterior border of the gland, identify and
transect the parotid duct
Remove the tumour with a cuff of the superficial parotid lobe
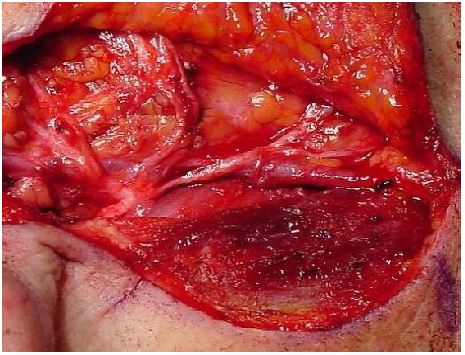
Parotid dissection for deep lobe tumours
The principles of resecting deep lobe tumours are to:
Identify, dissect and free up the facial nerve from the
underlying deep lobe or tumour, to provide access to the deep lobe.
This may involve either a superficial parotidectomy (Figure 22),
or simply reflecting the superficial lobe anteriorly, keeping the
parotid duct intact, and replacing it at the conclusion of surgery (Figure
23)
Deliver the tumour either between, or inferior to the facial
nerve or its branches, identifying the branches of the facial nerve
around the tumour, and removing tumour between the splayed facial nerve
branches (Figure 24)
Figure 22: Facial nerve has
been freed from
deep lobeFigure 23: Reflecting
superficial lobe for access to facial nerve
and to deep lobe tumourFigure 24: Tumour resected by
removing tumour
between splayed facial nerve branches
The deep lobe of the parotid/tumour is bordered medially by the
fat of the parapharyngeal space, and can be delivered from the
parapharyngeal space by blunt dissection
Be prepared to divide the external carotid, deep transverse
facial and superficial temporal arteries and the re-tromandibular and
superficial temporal veins if and when they are encountered during
dissection
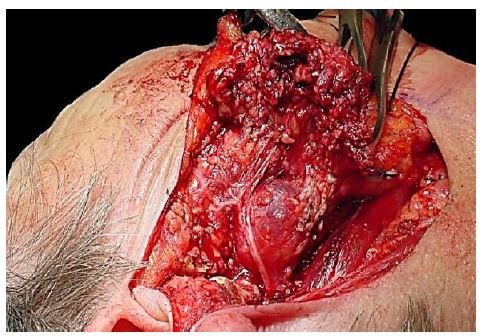
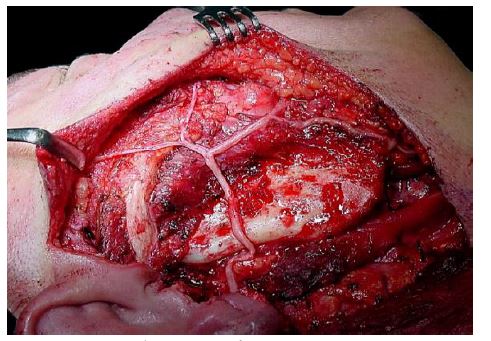
Additional access may be provided to the deep aspect of a tumour
by dividing the styloid process and/or via a transcervical approach (Figure
25)
Figure 25: Access to
parapharyngeal space tumour extension by
reflecting the superficial lobe and division of styloid processFigure 26:
Completed total parotidectomy in patient shown in Figure
22; silk ties are on branches of the external carotid artery
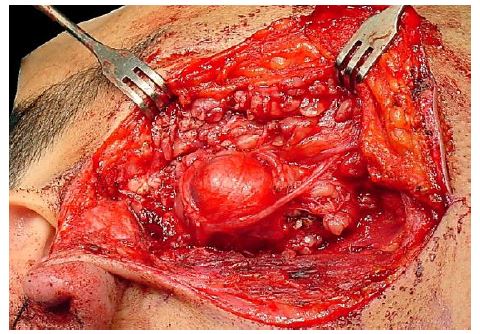
Tumour spillage
Great care should be taken to avoid rupture and spillage of
pleomorphic adenoma tis-sue into the operative site as it may lead to
multifocal tumour recurrence, often more than 20yrs following surgery (Figure
27). A minor controlled capsular rupture may be simply managed by
copiously irrigating the wound. With more extensive ruptures,
especially of a pleomorphic adenoma in the parapharyngeal space, some
would advocate postoperative radiation therapy. Due to the multifocal
nature of the recurrence, MRI is an important preoperative
investigation for recurrence. Having to operate in a previously
dissected field, the facial nerve is at greater risk of injury, and
should be monitored during surgery.
Figure 27: Multifocal
recurrence of pleomorphic adenoma
Wound closure
Confirm nerve continuity:Carefully
inspect the nerve. One may stimulate the nerve with a nerve stimulator.
Neuropraxia due to mechanical trauma may however cause failure of
muscle con-traction
Obtain meticulous haemostasis: Use ties
and bipolar diathermy. Employ a Valsalva manoeuvre to identify venous
bleeding
Sealed suction drain: Until drainage
<50ml/24 hrs
Skin closure: Subcutaneous and
subcuticular absorbable sutures
Facial nerve repair
Unlike with malignant tumours, the facial nerve and its branches can
virtually always be dissected free from benign neoplasms. Isolated
midfacial branches may be sacrificed without causing visible facial
dysfunction. Transection of the temporal (frontal) and marginal
mandibular nerves however results in disfiguring facial asymmetry;
these nerves should be repaired with 8/0 nylon/prolene epineural
sutures. When primary nerve repair is not possible due to undue tension
or nerve resection, then the nerve can be grafted with greater
auricular nerve, or sural nerve.
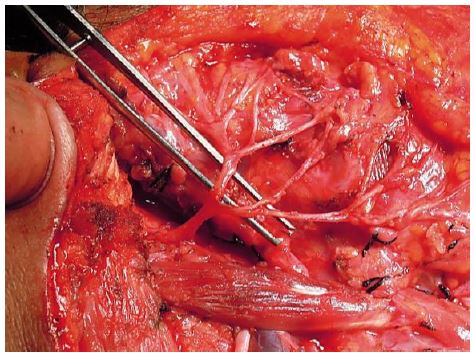
The greater auricular nerve is
approximately the same diameter as the facial nerve trunk, and has a
few branches that can be used to graft more than one facial nerve
branch (Figure 28).
Figure 28: Greater auricular
nerve
The sural nerve provides greater length
and more branches and is better suited to bridging longer defects and
for grafting to more peripheral branches (Figures 29, 30).
Figure 29: Sural nerve
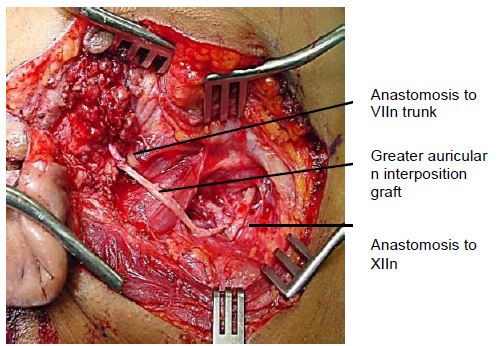
When the proximal end of the facial nerve is not available, e.g.
with extensive proximal perineural tumour extension, then a hypoglossal-facial
nerve interposition graft can be used to restore facial
tone and movement. The nerve graft is sutured end-to-end to the distal
facial nerve(s), and end-to-side to the hypoglossal nerve after cutting
about 25% into the side of the hypoglossal nerve to expose the nerve
axons (Figure 31).
Johan Fagan MBChB, FCORL, MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa johannes.fagan@uct.ac.za