RESECTION OF EXTRATEMPORAL PARAGANGLIOMAS INCLUDING CAROTID
BODY AND GLOMUS VAGALE TUMOURS
Johan Fagan & Vincent Vander Poorten
Paragangliomas, also known as glomus tumours or chemodectomas,
are
neuroendocrine tumours that originate from glomus cells in paraganglia.
They are derived from the embryonal neural crest. The cells are part of
the sympathetic nervous system and serve as chemoreceptors. They are
located in the vascular adventitia of blood vessels which include the
carotid bodies in the carotid artery bifurcation (Figure 1).
Figure 1: Carotid body within
carotid bifurcation; it
is equivalent to the size of a grain of rice (Khan Q, Heath D, Smith P.
Anatomical variations in human carotid bodies. J Clin Pathol.
1988;41:1196–99)
Paragangliomas occur within the skull base
(glomus jugulare, glomus tympanicum), the parapharyngeal space (carotid
body tumours, vagal paragangliomas), the larynx and the neck, as well
as in the chest and the abdomen. In the head and neck, the carotid body
location is most frequent, followed with decreasing frequency in
jugular, tympanic and vagal locations. The incidence and prevalence in
populations of these rare head and neck tumours remains unclear, as
most are benign tumours not captured by cancer registries. The reported
proportion of malignant paragangliomas is 6 - 19%. The malignant nature
is demonstrated only by imaging studies showing local invasion,
regional or distant metastasis, since the histological appearance of
malignant paragangliomas is identical to that of benign tumours. 1
Regarding the genetic basis of these tumours, about 90% of
paragangliomas are sporadic, but in 1 in 10 patients a mutation in the
gene coding for succinate dehydrogenase (SDH) subunits (SDHD, SDHB,
SDHC) is observed. These patients typically develop multifocal
paragangliomas already under 40 years of age, and also present with phaeochromocytomas.
The latter are neuroendocrine tumours of the adrenal medulla and are
closely related to paragangliomas. Unlike paragangliomas they are
chromaffin positive and hence secrete catecholamines.
This chapter focuses on the surgical management of
extratemporal
paragangliomas of the head and neck. Even though surgery remains the
mainstay of therapy for easily resectable paragangliomas, many of these
tumours are very slowly growing, or do not even grow at all; hence a
watchful waiting approach with serial imaging (“Wait and See approach”)
may be preferable. Another treatment modality to be considered is
irradiation.
Surgically relevant issues
Not all paragangliomas need surgery
On the one hand, an initial wait-and-scan policy
can be
justified for many patients based on the slow growth rate, with half of
tumours not increasing in volume during long-term follow-up. 2
In a recent study of cervical paragangliomas followed up for a mean of
5yrs (1-17ys), 42% tumours remained stable, 38% grew, and 20% reduced
in size. In those that grew, the mean growth was only 2mm p.a. 3
On the other hand, in documented volume-increasing lesions,
both radiotherapy and surgery
are valid options.
Radiotherapy can consist of Intensity
Modulated Radiotherapy (IMRT) using a moderate-dose of 44-50 Gy in
22-25 fractions 1, or stereotactic radiosurgery
4 in selected very small skull base lesions.
Although radiotherapy is not curative, 10 year local control
rates using RT of 94% and higher have been reported. 5, 6
Radio-therapy, however, is associated with a (<1%) risk of
radiation-induced malignancy, and the natural course of tumour growth
mentioned above does question whether the purported benefits of
radiation have in fact been overstated. Anyhow, this modality should -
like surgery - only be considered in paragangliomas with a documented
growth on serial scanning.
Given the potential complications, surgery
is best reserved
for limited paragangliomas where minimal morbidity is expected.
Typically these are the carotid body tumors that are classified as Shamblin
Group
I (small, easily dissected from the vessels) and Group II
(glomus
tumor partially surrounding the vessels – see below). The former
constitute 70% of paragangliomas. For all other tumors (Group III
carotid body tumors and vagal – jugular – tympanic paragangliomas),
iatrogenic postoperative cranial nerve deficits are hard to avoid. A
recent review estimated the prevalence of complications in surgically
treated carotid paragangliomas as 22% postoperative cranial nerve
deficits, 3% strokes, and 1% perioperative deaths. 7
Reviewing the literature on vagal and jugular paragangliomas, the same
authors concluded that on average 1 extra postoperative cranial nerve
deficit occurs per patient operated, which is much more than the 8
post-treatment cranial nerve deficits per 100 patients treated with
radiotherapy, at a comparable local control rate of 80-90% for both
modalities. The authors conclude that, compared to surgery,
radiotherapy results in comparable tumour control, but significantly
less morbidity. Choosing between the two modalities, one should
consider the patient’s age, tumour size and Shamblin type, observed
tumour growth and cranial nerve function at presentation, and
eventually catecholamine production, in order to maximally safeguard
quality of life.
Therefore, patients with paragangliomas without features of
malignancy, and in the absence of catecholamine induced chronic
hypertension and its negative long-term cardiovascular effects, should
be given the option of observation. This applies especially to patients
with high surgical or anaesthetic risk, or with asymptomatic vagal
paragangliomas where resection is certain to cause vagus nerve (and
probably also hypoglossal) paralysis.
Vascularity
The extreme vascularity of paragangliomas may make surgery
challenging. With intratemporal paragangliomas this manifests as
pulsatile tinnitus, and a red vascular mass may be visible behind an
intact tympanic membrane. In the neck it may manifest as a pulsatile
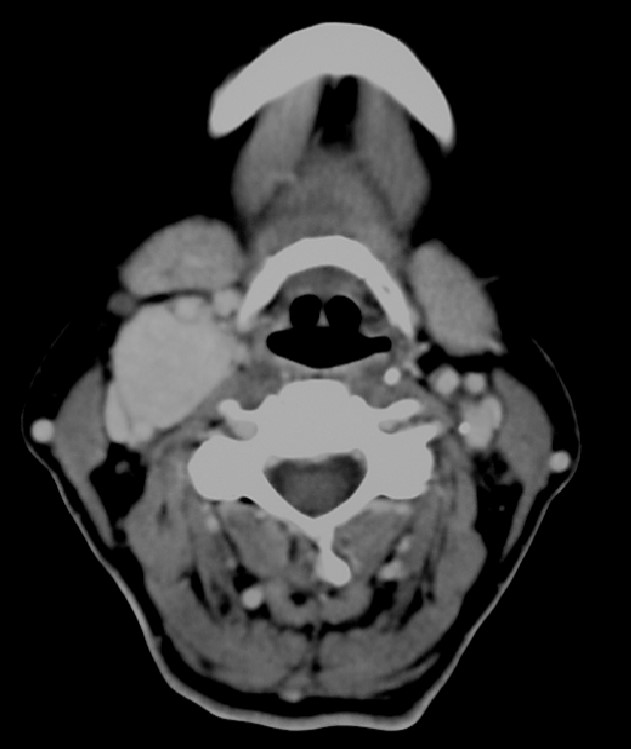
mass in the region of the carotid bifurcation. CT typically shows
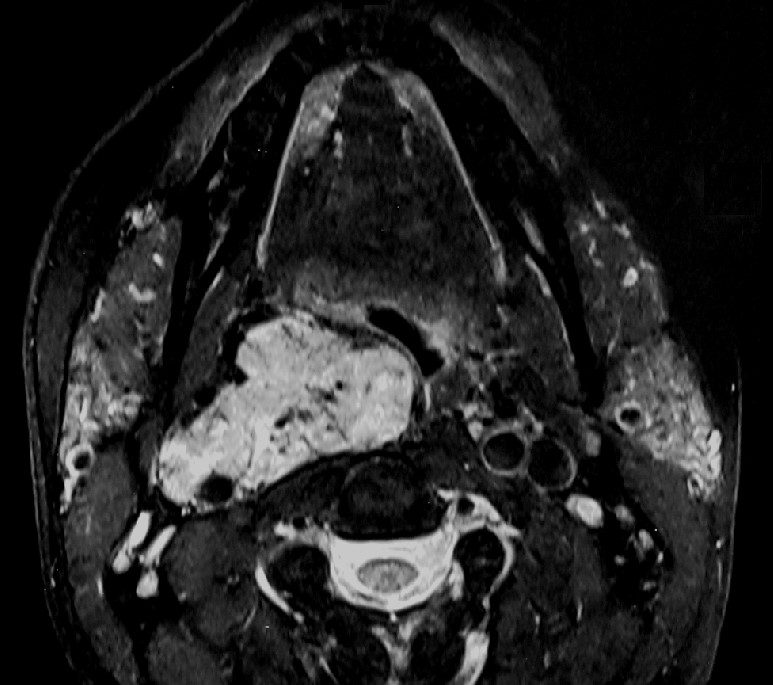
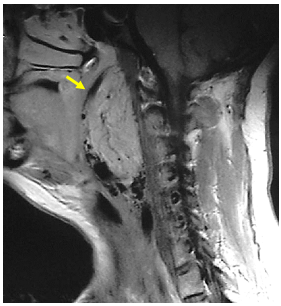
contrast enhancement (Figure 2) and signal flow
voids may be evident on MRI (Figure 3).
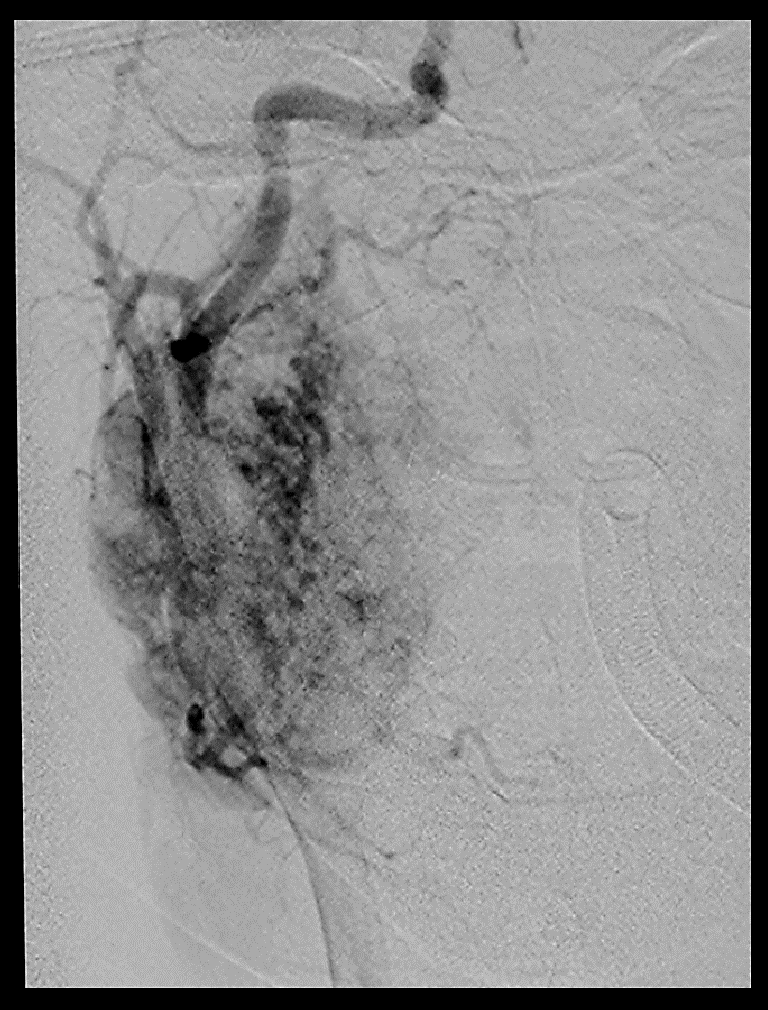
Angiography shows a rich vascular network (Figure 4).
Given the high diagnostic accuracy of modern imaging, attempts at
taking biopsies from these lesions is considered to be contraindicated.
Figure 2: Coronal CT scan shows
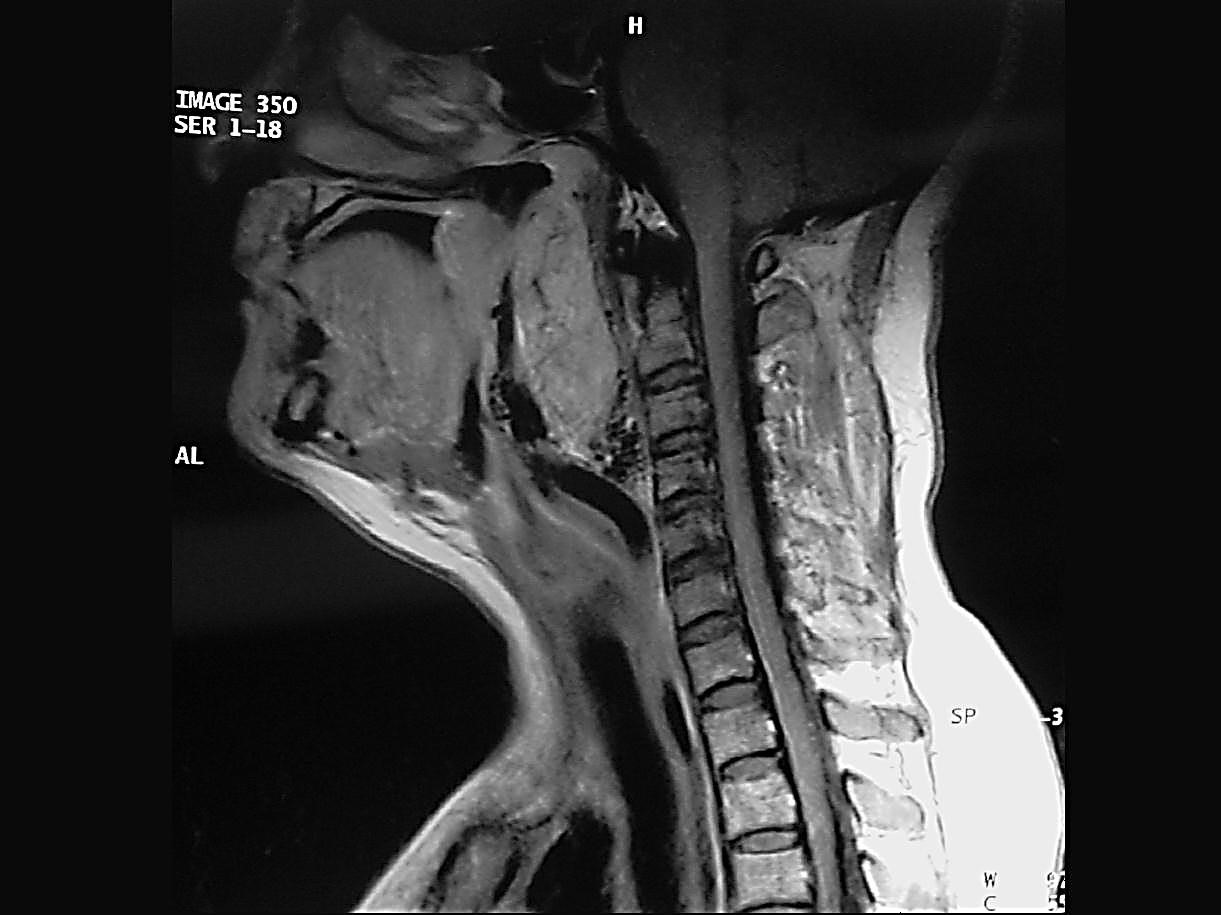
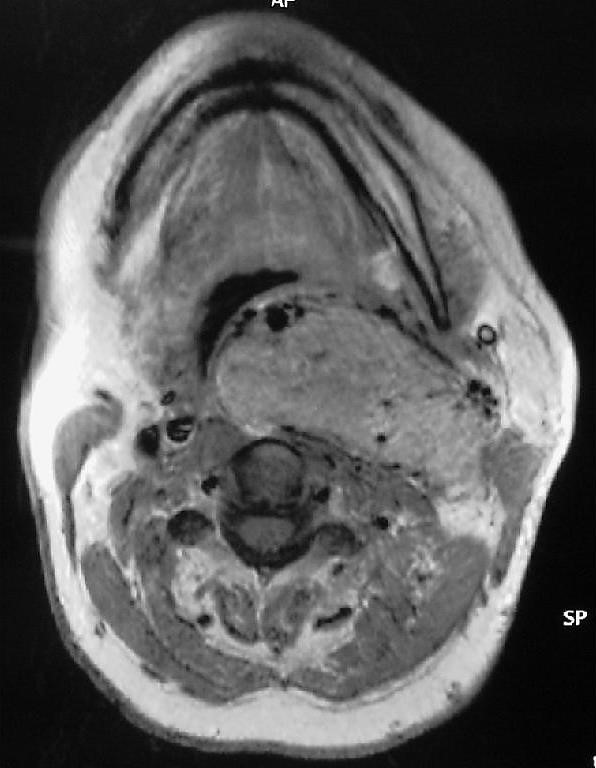
contrast enhancement of a carotid body tumourFigure 3: MRI shows (black) signal
flow voids of carotid vessels and smaller arteries within a carotid
body tumour
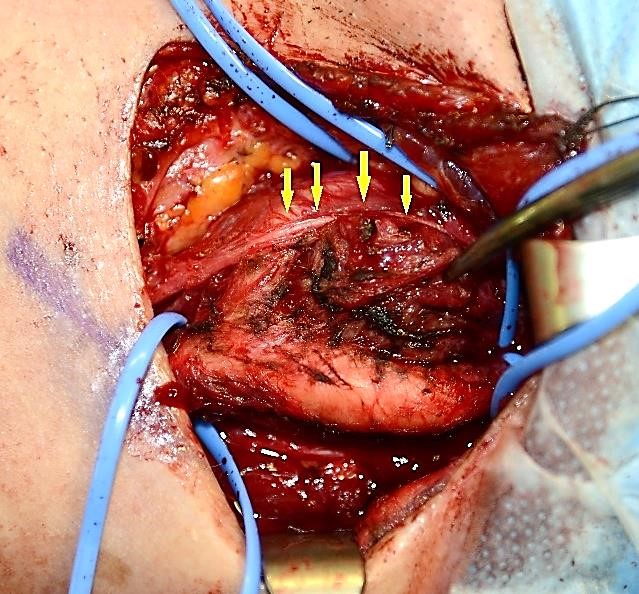
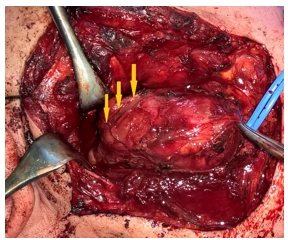
Lack of encapsulation
Especially with carotid body tumours, thin-walled vessels
cover the
surface of the tumour and blend with the adventitia covering the
carotid vessels. Because of their thin walls, monopolar cautery is
ineffective; hence the need to dissect the tumour from the carotid
arteries in a subadventitial plane and to control bleeding from the
multitude of thin-walled vessels with bipolar cautery or with multiple
ties (Figure 5).
Figure 4: Angiogram illustrating
vascularity of a carotid body tumourFigure 5: Bipolar cautery has been
used to achieve
haemostasis, and dissection is maintained in a subadventitial plane
(yellow arrows) on the internal carotid artery; retained adventitia
indicated by blue arrows (right neck)
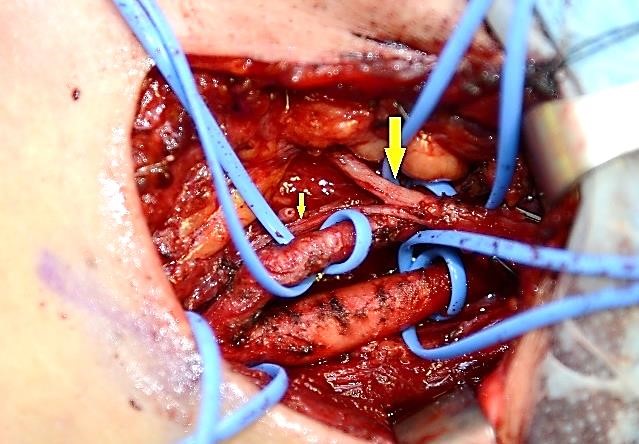
Nerves at risk of injury
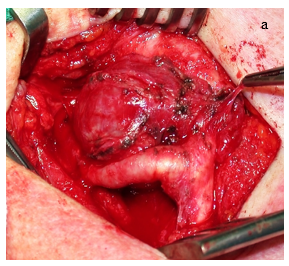
It is not uncommon for the hypoglossal (Figure 6a),
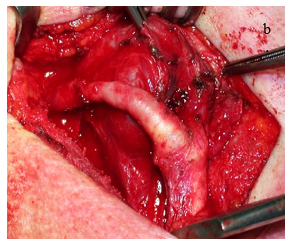
descendens hypoglossi (Figure 6b),
superior laryngeal, vagus, and accessory nerves and the sympathetic
trunk to be involved by a carotid body tumour. With glomus vagale
tumours the vagus nerve is at significant risk of permanent surgical
injury, but also the hypoglossal nerve and the sympathetic chain may be
embedded within a vagal paraganglioma. These nerves need to be
carefully identified beyond the confines of the tumour before
commencing the tumour resection so that they can be dissected free and
preserved if at all possible.
Figure 6a: After vessel-loop
control of the common,
internal and external carotid arteries, subadventitial dissection of
this right sided Shamblin type I carotid body tumour proceeds using
bipolar cautery; arrows indicate descends hypoglossi branch to ansa
cervicalisFigure 6b: Situation after removal
of the tumour shows
the preserved hypoglossal nerve (big arrow) and descendens hypoglossi
(small arrow)
Catecholamine secretion
Phaeochromocytoma-like symptoms due to catecholamine secreting
tumours occur in 1–3% of patients with paragangliomas in the head and
neck, and manifest with palpitations, hypertension, headaches, and
sweating. If left unattended, heart failure and arrhythmia will ensue
in the long run. Failure to detect catecholamine secretors can lead to
life-threating haemodynamic instability during embolisation or surgery.
Perioperative optimisation includes adrenergic receptor blocking
agents. Hence the need to test for free catecholamines so that
secretors can be optimised preoperatively. Alternately one can test for
urinary metanephrine levels or urinary vanillylmandelic acid (VMA)
levels (least expensive, but least specific). Because secreting
paragangliomas in the head and neck are so uncommon, raised
catecholamines should prompt one to exclude the presence of a
phaeochromocytoma. Proton pump inhibitors may cause false positive
elevation of serum chromogranin A; if elevated, PPIs should be
discontinued for a week and the test repeated.
Genetic screening
A family history is associated with increased likelihood of
multiple
paragangliomas and of patients presenting at an earlier age. There are
various genetic mutations of which 10% are hereditary.8
Patients with a positive family history and those with
multiple
paragangliomas must be offered genetic testing, although nowadays it
could be argued that all patients deserve genetic testing as often an
SDH mutation is found despite a negative family history. Paragangliomas
also occur in MEN syndromes types 2A and 2B.
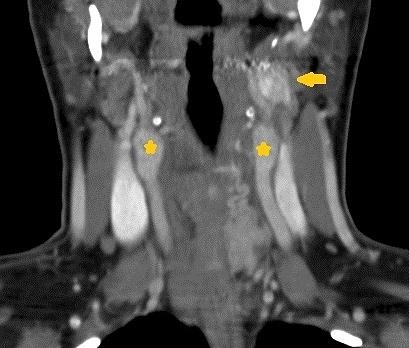
Multiple paragangliomas
About 10% of carotid body tumours are bilateral. Multiple
paragangliomas should be suspected in patients with a positive family
history and with head and neck paragangliomas that have raised
catecholamines (Figure 7).
Figure 7: Bilateral carotid body
tumours (*) and left
vagal paraganglioma (arrow) in a patient with a SDH-D mutation.
Following this diagnosis the patient’s brother was also diagnosed with
an SDH-D mutation and multiple paragangliomas
Radiological investigations
Radiological investigations may determine the following:
Confirm that it is a paraganglioma
CT, MR and MR angiography of the head and neck have such
typical
findings, that they obviate the need for a (hazardous) biopsy. Imaging
studies reveal the location, extent, relation to the great vessels, and
unsuspected coexistent paragangliomas at other sites.
CT with contrast
typically shows a hyperaemic mass (Figures 2, 8).
A small paraganglioma may however not enhance if peak-tumour
opacification is mistimed; the mass may then be mistaken for a
schwannoma or a lymph node. Metastatic papillary carcinoma of the
thyroid may also enhance with contrast.
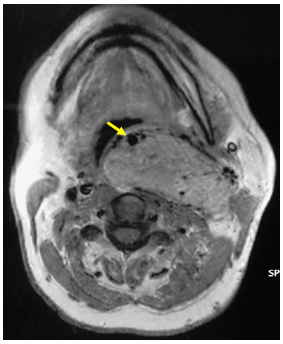
MRI reveals
a hyperaemic mass with signal flow voids on T2 (Figures 3,
9b) sometimes giving a classic salt-and-pepper
sign.
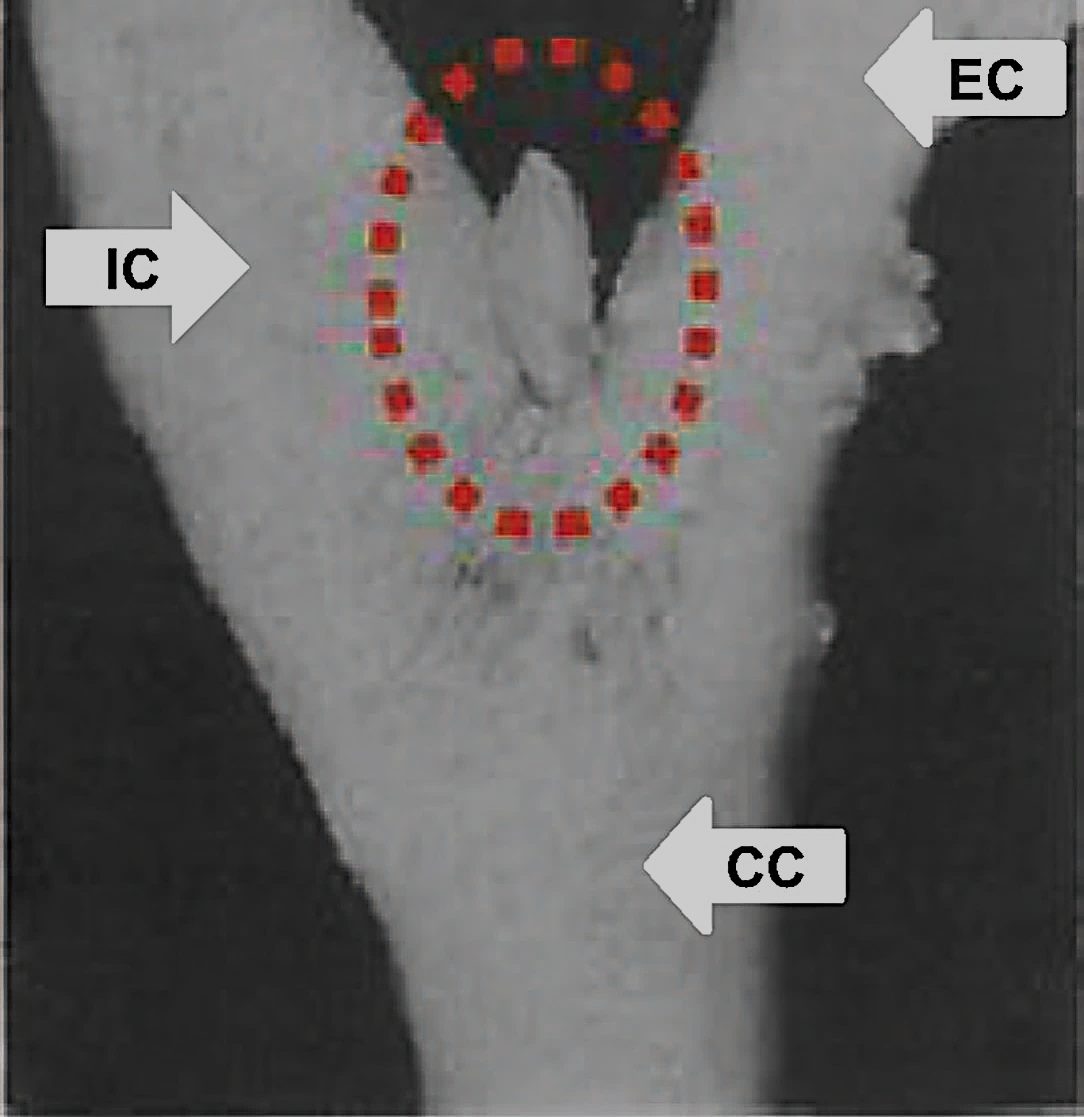
Carotid body tumour vs. vagal paraganglioma
Carotid body tumours classically splay the internal and
external carotid arteries (Lyre sign) (Figures 8a, b);
vagal paragangliomas displace the internal and external carotid artery
anteriorly (Figures 9a, b).
Figure 8a: Splayed carotid
bifurcation (Lyre sign)Figure 8b: Carotid body tumours
splay the internal and external carotid arteriesFigure 9a: Vagal paraganglioma
displacing the internal carotid artery anteriorlyFigure 9b: Vagal paraganglioma
typically displaces the internal carotid artery anteriorly
Resectability
Resectability is largely determined by the degree of
involvement and
encasement of the common and internal carotid arteries. Preoperative
classifications however have limitations as tumour adherence to the
carotid can ultimately only be determined at surgery during
subadventitial dissection.
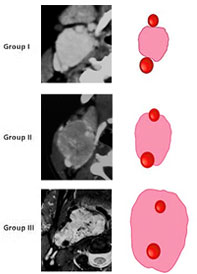
The Shamblin classification(Figure
10) groups carotid body tumours according to the degree of
encasement of the carotid vessels. Group I
tumours are minimally attached to the carotids and are easily resected.
Group II
tumours partially surround the carotids, are generally more adherent to
the adventitia and more difficult to resect, though still amenable to
subadventitial resection. Group III tumours
encase the entire
circumference at the carotid bifurcation; surgical dissection may be
impossible and is more likely to require sacrifice and grafting of the
internal carotid. As stated above, nonsurgical treatment e.g.
radiation therapy should be considered for Group III tumours; in the
event that surgery is elected, it may be prudent to do an angiogram to
check cerebral crossflow, and the surgeon should be experienced, and a
vascular surgeon should be on standby.
Figure 10: Shamblin classification
of carotid body
tumours; all 3 tumours on the left were resected without vascular
complications
Surgical relationship to carotid vessels
CT or MRI is employed to determine the position of the
internal and
external carotid arteries relative to the mass to provide a roadmap for
the surgeon to plan a surgical approach.
Multiple paragangliomas
Additional paragangliomas may influence management and should
be
suspected in patients with a family history, and with head and neck
paragangliomas that have raised catecholamines. They may be detected by
imaging studies e.g. ultrasound, CT, MRI or
angiography. A
somatostatin receptor scan (octreotide scan) can also be very useful to
assess the entire body to detect multiple paragangliomas.
Principal feeding vessel(s)
The ascending pharyngeal artery is generally the principal
feeding
vessel for carotid body tumours. Some surgeons prefer to have the
artery embolised preoperatively to facilitate the resection.
Stroke risk with occlusion of common or internal carotid
artery
When concerns exist that cerebral blood flow may be
interrupted when
resection necessitates division of the common or internal carotid
arteries, then preoperative angiography (with balloon occlusion test to
check for patency of the Circle of Willis) may be employed to check the
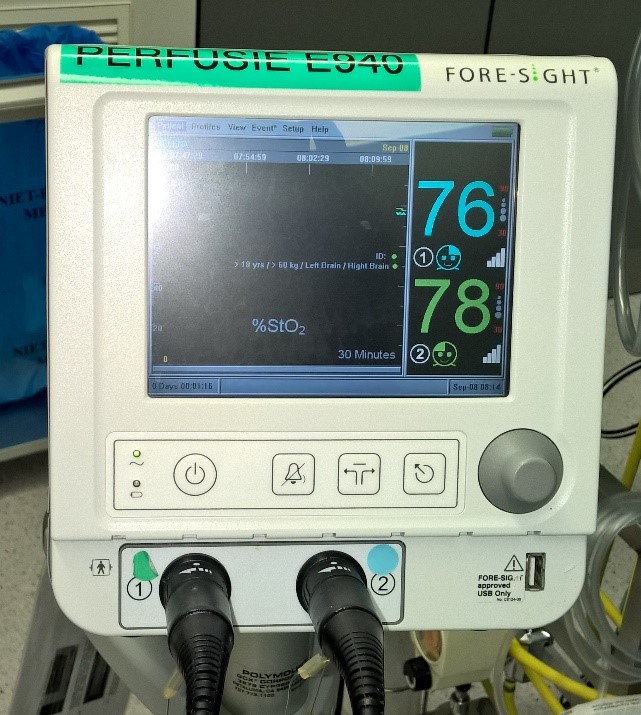
degree of cerebral crossflow. When available, it is recommended to use
perioperative brain oxygen saturation monitoring (Figure 11)
Figure 11a: Electrodes placed on
patient’s forehead to monitoring brain oxygenation using the ForeSight
systemFigure 11b: Symmetry of oxygenation
can be followed throughout the procedure using the ForeSight system
Clinical presentation
Cervical mass
Generally a non-tender asymptomatic mass; vagal
paragangliomas may be more cephalad
Mobile in transverse, but not vertical planes
May be pulsatile and have a bruit
May extend cephalad within the poststyloid
parapharyngeal space to
the cranial base and medially displace the lateral pharyngeal wall
May produce vague pain, hearing loss, pulsatile
tinnitus
Bilateral (10% carotid body tumours)
Nerve palsies in about 10%
Cranial nerves IX (velopharyngeal insufficiency), X
(hoarseness, aspiration), XI (shoulder weakness), XII)
Horner’s syndrome
Phaeochromocytoma-like symptoms: up to 3% secrete
catecholamines
Preoperative assessment
Is it a paraganglioma?
Family history
MEN type 2A and 2B
Imaging (do not required all three)
CT with contrast
MRI
Angiography
Is it secreting or non-secreting?
24-hour urinary catecholamines and metanephrines
Plasma metanephrine if at high risk e.g.
predisposing genetic syndromes, family history of phaeochromocytoma)
If secreting
Exclude phaeochromocytoma
Refer to physician or anaesthetist for pre- and
perioperative optimisation including adrenergic receptor blocking agents
Has a “Wait and scan” strategy demonstrated growth?
Is it resectable – what is the Shamblin group?
Is it malignant?
Is the patient a good surgical candidate?
What alternative management is available?
Are there other paragangliomas?
Ultrasound neck and abdomen
CT / MRI of skull base to abdomen
MIBG scan
If for surgery
Possible consequences and complications?
What side to operate on 1st
with bilateral carotid body tumours?
Generally operate on easier side as less likely
to cause cranial nerve complications
If have cranial nerve complication, then still
have the option to observe or irradiate the 2nd
side
What is the position of the carotid vessels
relative to the tumour?
Important for planning the surgical approach
and performing the surgery
Contrasted CT / MRI / angiogram
Should the tumour be embolised preoperatively?
Conflicting views among surgeons about benefits
of embolisation
Potential for neurological complications
Greatest theoretical value with large tumours
Most commonly embolise the ascending pharyngeal
artery
What is the cerebral crossover blood flow like
should the common or
internal carotid artery have to be sacrificed? Should this be a concern
it can be determined by angiography +/- balloon occlusion tests
Surgical approaches
The principal challenges relating to post-styloid masses are
avoiding injury to the internal carotid artery, internal jugular vein
and the lower cranial (especial XII) and sympathetic nerves. Access is
limited by the vertical ramus of the mandible, the parotid gland, the
facial nerve and the styloid process with its muscular and ligamentous
attachments.
Carotid and vagal paragangliomas are located in the
poststyloid
parapharyngeal space and are initially approached via the transcervical
approach; additional anterior exposure is achieved by a
transcervical-submandibular approach; and additional superior access is
achieved by including the transparotid approach (Figures 12,
22). (See chapter Access
to Parapharyngeal Space).
Patients should therefore always be consented for transcervical and
transparotid approaches. The authors have never had to resort to a
mandibulotomy.
Patients should be cautioned about the sequelae of vascular
and
lower cranial nerve injury, as well injury to the sympathetic trunk
causing Horner’s and “1st Bite” syndromes.
Anaesthesia
Oral or nasal endotracheal intubation
Avoid muscle relaxants so that cranial nerves VIIX, XI, XII
can be monitored
No antibiotics unless pharynx is entered
Routine anaesthetic monitoring unless a secreting
paraganglioma
If a secreting tumour
Ensure that adrenergic system was adequately blocked in
the preoperative phase
Monitor blood pressure with arterial line
Have appropriate drugs available to control blood pressure fluctuations
Blood: either Grouped and Screened, or cross matched
Brain oxygenation can be monitored particularly with
Shamblin 3 tumour resections (Figures 12 a, b)
Surgical equipment to have available
Bipolar electrocautery
Vascular sutures and vascular loops to place around vessels
and nerves
Vascular forceps
Lahey vascular clamp (Figure 13)
Figure 13: Lahey vascular clamp
Surgical technique
Place the patient supine with neck extended and turned to
the opposite side
Inject local anaesthetic with 1/100000 adrenaline along the
incision line, especially preauricularly
Sterilise the face and neck
Drape the patient but keep the corners of the mouth and eye
exposed
to monitor facial movement if a transparotid approach is to be employed
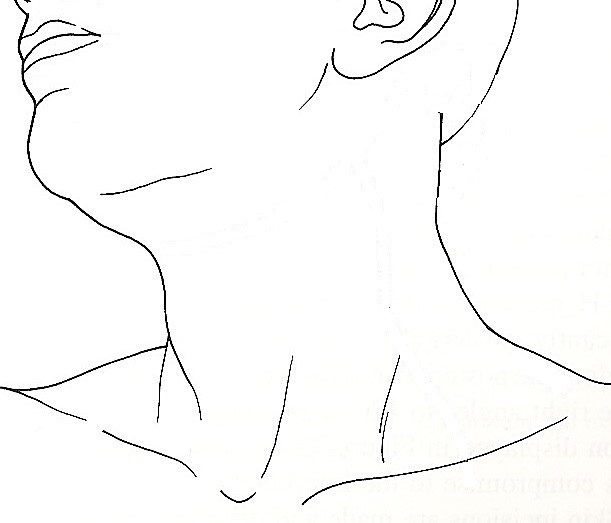
Open the neck as indicated in Figure 14. The
incision for
the transcervical approach is made at the level of the hyoid bone. The
parotid incision may be delayed until it is found that the
transcervical approach does not provide adequate access
Figure 14: Skin incisions: Green
for transcervical +/- submandibular approach; add red incision for
transparotid approach
Transcervical approach(Figure
15)
The transcervical approach is suited to paragangliomas
extending up to the level of the styloid process
Expose the upper neck via a transverse skin crease incision
at the level of the hyoid bone (Figure 14)
Extend the skin incision posteriorly over the
sternocleidomastoid muscle
Divide the platysma muscle taking care not to injure the
greater auricular nerve which should be preserved
Ligate and divide the external jugular vein just anterior
to the greater auricular nerve to improve access to the upper neck
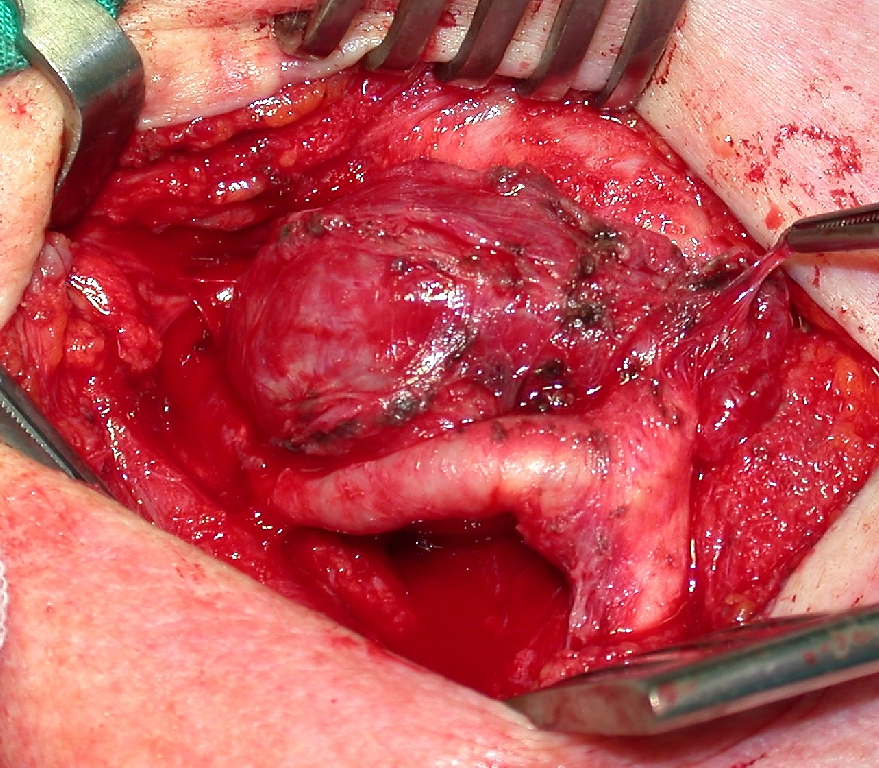
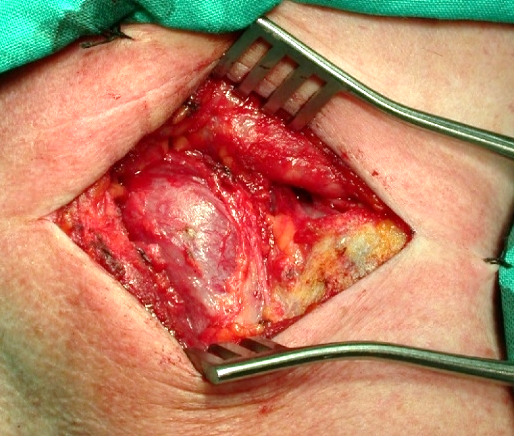
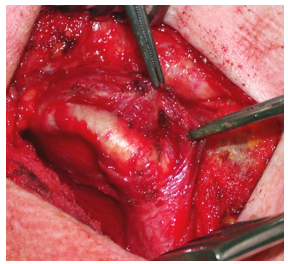
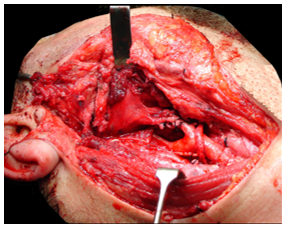
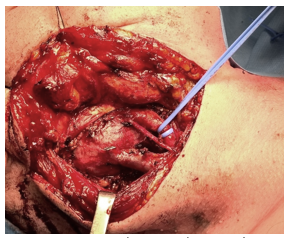
Identify the paraganglioma, taking care not to traumatise
its thin-walled surface vessels (Figure 15)
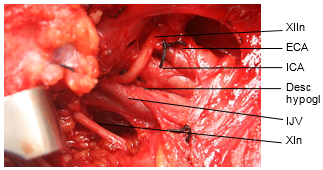
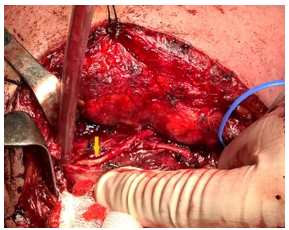
Proceed to identify as many of the following anatomic
structures around the paraganglioma (Figure 16)
Common carotid artery
Carotid bifurcation
Internal carotid artery
External carotid artery
Internal jugular vein
Posterior belly of digastric muscle
Hypoglossal nerve
Descendens hypoglossi
Vagus nerve
Accessory nerve
Sympathetic trunk
Superior laryngeal nerve
One may opt to place vascular loops around the major
vessels for vascular control should a vascular injury occur (Figure 6)
Use a combination of sharp dissection and bipolar
cautery to
dissect nerves free that are trapped in the surface of the mass, most
commonly the hypoglossal nerve (Figure 17)
Figure 15: Carotid body tumour
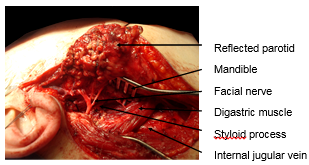
exposed in right neckFigure 16: Structures around a
paraganglioma; the sympathetic trunk is found on the posterior aspect
of the carotid sheathFigure 17: XIIn and descendens
hypoglossi running in the surface of the paraganglioma, having to be
dissected free
Next direct your attention to the periphery of the mass at
the
common, internal or external carotid arteries or the carotid bifurcation
Establish a subadventitial dissection plane on the artery (Figure
18)
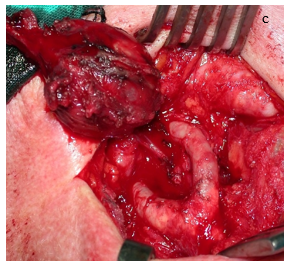
Dissect the mass off the arteries with scissors keeping in
this subadventitial plane (Figures 18, 19, 20)
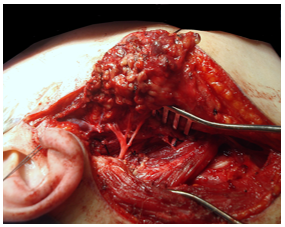
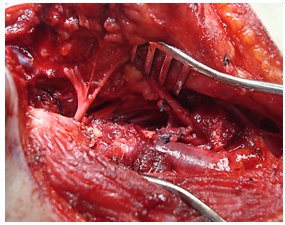
Figure 18: Freeing the
paraganglioma from the internal carotid artery in a subadventitial
dissection plane Figure 19a, b, c: Freeing the
paraganglioma from the carotid bifurcation and external carotid artery
in a
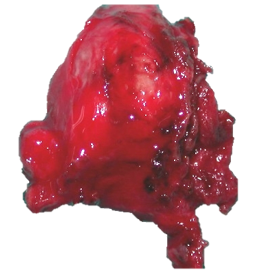
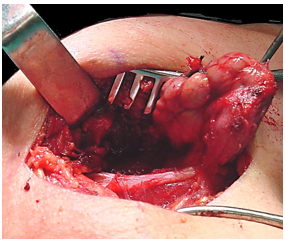
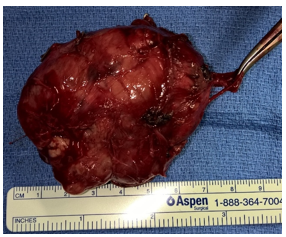
subadventitial planeFigure 20: Resected carotid body
tumour
Surgical tips
Identify and preserve the nerves listed above during the
course of the dissection
Maintain a dry surgical field at all times by using bipolar
cautery and ties for haemostasis
Avoid excessive cautery on the carotid wall as this may
weaken the
artery and cause it to rupture; also in the post-operative phase a
pseudoaneurysm may form and only rupture days later
Avoid excessive manipulation or rotation of the carotid
vessels as
this may cause thrombosis or release plaque or emboli causing a stroke
Be very careful not to injure the arterial wall when
dissecting within the carotid bifurcation
The surgeon may elect to divide and ligate or oversew (with
proline) the external carotid artery and to resect external carotid
artery with the tumour; avoid dividing the artery close to the
bifurcation as it is more difficult to ligate the artery at this point,
there may be plaque at the bifurcation, and the
artery may
tear if ligated too close to the bifurcation
Be prepared to have to repair the carotid vessels if
traumatised,
so have vascular sutures, vascular forceps and a Lahey vascular clamp
available in the operating room (Figure 21).
Depending on your own experience it may be prudent to have your
vascular surgical colleague on standby
Figure 21: After subadventitial
dissection the remaining carotid wall was too thin and the risk of
subsequent aneurysmic blow-out was judged too high; hence the common
carotid (vertical arrow) to internal carotid (horizontal arrow) was
replaced with a Dacron ® interposition graft and the external carotid
was ligated. During this procedure the ForeSight system ® provided
information of the patency of the circle of Willis and brain
oxygenation. The patient did well postoperatively
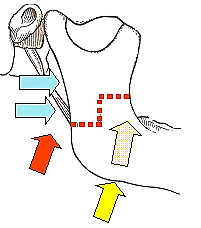
Gaining additional exposure(Figure 12)
Additional exposure may be achieved by adding one or more of
the following approaches to the transcervical approach:
Transecting posterior belly of digastric muscle
Transparotid approach
Transcervical-submandibular approach
Mandibulotomy of vertical ramus
Transecting posterior belly of digastric
The posterior belly of the digastric muscle may either be
retracted
superiorly or divided to provide additional access medial to the
parotid gland and the facial nerve
Take care not to injure the facial nerve as it bifurcates
the angle between the styloid process and the digastric muscle
Transparotid approach
Figure 22a, b: Transparotid access
Elevate the superficial lobe of the parotid gland off the
trunk of the facial nerve up to the pes anserinus
and retract the gland anteriorly (Figure 22)
Free the facial nerve from the deep lobe of the parotid
gland
Excise the deep parotid lobe in the retromandibular sulcus (Figure
22)
This exposes the styloid process
Immediately deep to the styloid are the contents of the
poststyloid PPS including the internal carotid artery
Access can be further improved by excising the styloid
process with
a bone nibbler, dividing the stylomandibular ligament, and retracting
the mandible anteriorly (taking care to avoid excessive tension on the
facial nerve), and inferiorly by dividing the posterior belly of the
digastric and “styloid muscles” (Figures 23, 24)
Figure 23: Additional access by
transecting digastric muscle and styloid apparatusFigure 24: Wide access to PPS
following resection of large glomus vagale tumour
Transcervical submandibular approach(Figure 25)
Tumours extending anteriorly may require combinations of
transparotid, transcervical and transcervical submandibular approaches.
Transecting the posterior belly of the digastric muscle and/or the
“styloid muscles” further improves access.
Figure 25: Additional access by
dividing the facial artery where it appears above digastric, and
displacing submandibular gland anteriorly
Closure
Insert a closed suction drain
Close the skin in a normal fashion
Postoperative care
Remove suction drains when <50ml drainage / 24 hrs
Check that patient swallows without aspirating before
introducing oral feeding
Complications
Haematoma
Cranial nerve injuries VII, IX, X, XI, XII
Sympathetic trunk injury
First bite syndrome
Horner’s syndrome
Cerebrovascular accident
Carotid artery injury causing false aneurysm or blowout
Glomus vagale / vagal paraganglioma
Unlike carotid body tumours, glomus vagale tumours generally
displace the carotid vessels anteriorly (Figures 26, 27, 28).
They may extend through the skull base as a dumbbell tumour. Therefore
imaging to demonstrate the anatomical relationship of the internal
carotid artery to the mass is essential to permit surgical planning and
to safely perform the surgery.
Because the vagus nerve is generally sacrificed with the resection (Figure
28d), some patients may elect to adopt a watchful waiting
approach to preserve voice function for as long as possible.
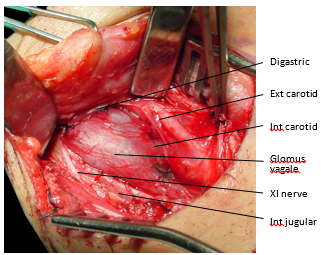
Figure 26: Glomus vagale tumour
located between the internal jugular vein and the internal carotid
artery Figure 27a, b: Glomus vagale tumour
displacing the internal carotid artery (yellow arrow) anteriorlyFigure 28a: Secreting glomus vagale
tumour between carotid artery and jugular vein; descendens hypoglossi
nerve visibleFigure 28b: Dissecting the XIIn out
of glomus vagale tumour capsuleFigure 28c: Glomus vagale tumour
being removed; note groove from which XII nerve was dissected (arrows)Figure 28d: Resected specimen of
secreting glomus vagale tumour with the clamp holding the transsected
vagus nerve
References
Mendenhall WM, Amdur RJ, Vaysberg M, Mendenhall CM, Werning
JW. Head and neck paragangliomas. Head Neck
2011;33:1530-4 van der Mey AG, Frijns JH, Cornelisse CJ et al. Does
intervention improve the natural course of glomus tumors? A series of
108 patients seen in a 32-year period. Ann Otol Rhinol
Laryngol 1992;101:635-42
Foote RL, Pollock BE, Gorman DA et al. Glomus jugulare
tumor: tumor control and complications after stereotactic radiosurgery.
Head Neck 2002;24:332-8
Verniers DA, Keus RB, Schouwenburg PF, Bartelink H.
Radiation
therapy, an important mode of treatment for head and neck
chemodectomas. Eur J Cancer 1992;28A:1028-1033
Suarez C, Rodrigo JP, Bodeker CC et al.Jugular
and vagal paragangliomas: Systematic study of management with surgery
and radiotherapy. Head Neck 2013
Aug;35(8):1195-204
Suarez C, Rodrigo JP, Mendenhall WM et al. Carotid body
paragangliomas: a systematic study on management with surgery and
radiotherapy. Eur Arch Otorhinolaryngol 2014
Jan;271(1):23-34
Martin TP, Irving RM, Maher ER. The genetics of
paragangliomas: a review. Clin Otolaryngol
2007;32:7-11 vincent.vanderpoorten@uzleuven.be
Author & Editor
Johan Fagan MBChB, FCORL, MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa johannes.fagan@uct.ac.za
Author
Vincent Vander Poorten MD PhD MSc
Professor
Otorhinolaryngology, Head & Neck Surgery
University Hospitals Leuven
Department of Head and Neck Oncology
KU Leuven, Belgium