
Clinical presentations and epidemiology: Roughly 7% of HIV-infected persons present with telogen effluvium presenting as diffuse alopecia. The other findings include lengthening of the eyelashes, fine texture and straightening in late-stage disease. The hair also breaks more easily.
Aetiology and Treatment: The mechanism is thought to be multifactorial including nutritional deficiency, as a result of scalp inflammatory disorders like seborrheic dermatitis and autoimmune apoptosis of stem cells in the hair follicle. Alopecia, involving the scalp, has been reported inpatients with HIV infection treated with indinavir and lopinavir/ritonavir. The alopecia will generally reverse after substituting the offending drug(s).
Nail abnormalities are reported twice as often in HIV-infected persons compared to the normal population.
The most common nail abnormality in HIV is onychomycosis occurring in a third of patients. It often presents with uncommon forms, namely proximal or superficial onychomycosis. There is often co-infection with mold fungi or candida.
Melanonychia is the darkening of the finger and toe nails. In HIV-infected individuals, it is characterized by longitudinal hyper pigmented linesin the nails. The increase in nail pigmentation is caused by amplified pigment production by melanocytes due to activation of nail matrix melanocytes.Longitudinal melanonychia associated may be associated with treatment by zidovudine.
Other features that are significantly more common in HIV include transverse ridging, clubbing, splinter hemorrhages, absence of lunula, periungual erythema and proximal or total leukonychia.
Susceptibility to antifungal therapy is normal butonychomycosis in HIV-infected patients is more difficult to treat, probably as a result of co-infections. Thus, it is important to select a broad-spectrum antifungal therapypossibly for extended periods. There is no specific therapy for the other conditions except antiretroviral therapy.
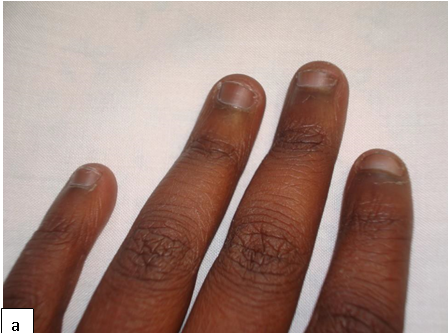


Digital clubbing has been described in various pulmonary, cardiovascular, infectious, hepatobiliary and gastrointestinal diseases. It is characterized by bulbous enlargement of the distal phalanges due to an increase in soft tissue. Common causes of digital clubbing include cyanotic heart disease, neoplasms of the lungs, pulmonary tuberculosis, bronchiectasis, liver cirrhosis, and inflammatory bowel disease.
Its presence in concomitant HIV disease may be caused by lymphoid interstitial pneumonitis (LIP) or chronic lung disease.