
The most common conditions in this group are seborrheic dermatitis, xerosis and papular eruptions.
Moisturisers and emollients may be useful in certain conditions discussed in this section. They help sooth and hydrate the skin and include oil instilled in the baths (e.g. liquid paraffin) and creams (e.g. Cetomacrogol cream). Lotions and ointments (emulsifying ointment or humectants such as 5-10% Urea contained in emulsifying ointment) are also available to be applied directly to the skin but are reserved for applications to very dry skin.
Topical corticosteroids (applied to the skin as cream or ointment) used as anti-inflammatory agents are subdivided into seven groups, with group one being the most potent and group seven the least potent (WHO model prescribing information- Drugs used in skin diseases. Geneva, World Health Organization, 1997).
Group 1: Super high potency e.g. clobetasol propionate 0.05%.
Group 2: High potency e.g. betamethasone diproprionate 0.05%.
Group 3: Upper-mid potency e.g. mometasone furoate 0.1% ointment.
Group 4: Mid potency e.g. mometasone furoate 0.1% cream.
Group 5: Lower-mid potency e.g. betamethasone valerate 0.1%.
Group 6: Mild potency e.g. fluocinolone acetonide 0.01%.
Group 7: Least potent e.g. hydrocortisone 1%.
Definition: Recurrent and often chronic hypersensitivity reaction to insect bites.
Aetiology: The reaction results from mosquito, flea, bedbug and other insect bites in hypersensitized children.
Epidemiology: Papular urticaria is predominantly a disease of children although it also occurs in non-local adults. It is thought to affect adults who have not been desensitized by previous recurrent bites by the same insects. It is a self-limiting condition and the children tend to outgrow the disease.
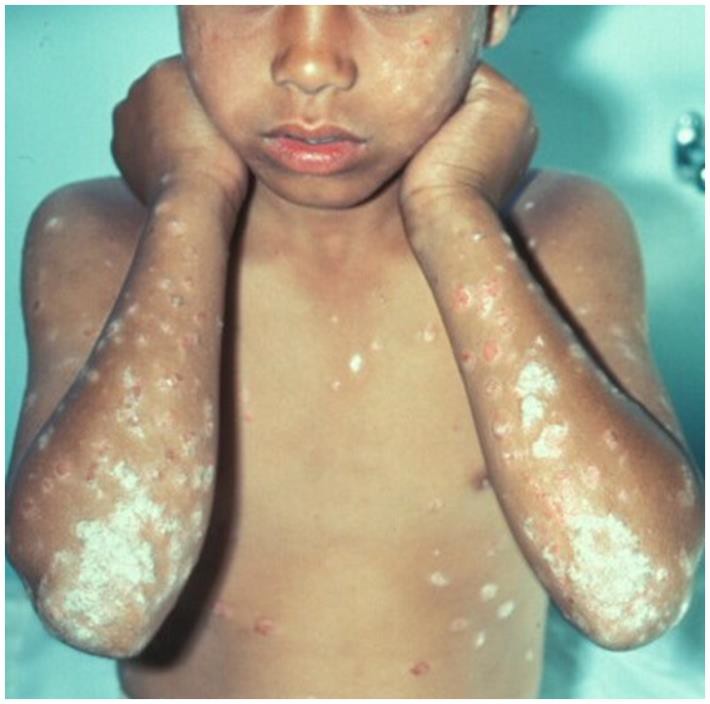
Clinical presentation: It presents as intensely pruritic papules that may be surrounded by a wheal. In severe cases blisters may form. The lesions tend to occur in groups or clusters in exposed and covered parts of the body. Scratching may result in excoriation and dyspigmentation. In recurrent cases, the lesions are usually in different stages of evolution.
Diagnosis: Papular urticaria is a clinical diagnosis. A skin biopsy is helpful in supporting the diagnosis in difficult cases.
Prevention: Insect repellents and insecticides help prevent insect bites.
Treatment: This is mainly symptomatic and topical steroids (e.g. 1% Hydrocortisone cream) and antihistamines (e.g. Chlorpheniramine) are helpful.
Complications: secondary bacterial infections.


HIV-related pruritic papular eruption (PPE) and eosinophilic folliculitis (EF) are poorly differentiated and are confused in their diagnosis.
Description: Papular pruritic eruptions (PPE) are a common dermatological manifestation of HIV and may often be the may often be the first sign of HIV which could be useful in diagnosing the infection. PPE is a sign of advanced degree of immunosuppression, occurring at low CD4 T-cell counts. The severity of PPE increases as CD4 counts decrease.
PPE has a clinical overlap with eosinophilic folliculitis (EF) of HIV.
Epidemiology: PPE prevalence varies between 10 and 60% depending on geographical area. It is common in Africa and Asia.
Aetiopathogenesis: PPE is postulated to be due to altered and exaggerated immune response to arthropod antigens as a result of the increased involvement of exposed or uncovered skin. It is associated with eosinophilia and elevated IgE.
Clinical presentation: PPE presents as chronic waxing and waning, intensely pruritic papules and symmetric involving predominantly the extremities and trunk, though facial involvement can also occur. The mucous membranes, palms and soles are spared. Extensive excoriation with subsequent scarring and post-inflammatory hyperpigmentation from scratching and infection can be disfiguring and stigmatizing.
Diagnosis: Skin biopsy is helpful to diagnose both EF and PPE. PPE histology shows a wedge-shaped, moderately dense, superficial and deep perivascular and interstitial lymphocytic and eosinophilic infiltrate; the epidermis is hyperplastic and there may be a spongiotic punctum.
Differential diagnosis: Differential diagnosis of both PPE and EF include nodular prurigo, prebullous pemphigoid, scabies, papulonecrotic tuberculid, drug eruption, photodermatitis, secondary syphilis, onchodermatitis and eosinophilic, pityrosporum, bacterial and acneiform folliculitis.
Treatment: It is a strong clinical indication for initiating ART. Initiation of ART has been shown to dramatically decrease the severity of PPE-HIV, often with lesions disappearing and not returning. Treatment of PPE is similar to that of eosinophilic folliculitis. Topical steroids, antihistamines, phototherapy and pentoxifylline (oxpentifylline) have been claimed to be efficacious.
EF is common among HIV-infected children. It is a marker of CD4 decline. The cause of EF is unknown. It is thought to be a result of immune dysregulation to a variety of agents such as Pityrosporum ovale, or the follicular mite Demodex folliculorum, an autoimmune reaction to the sebocyte, or a component of sebum.
Clinical presentation: EF has characteristic morphology and distribution, resembling insect bites. EF presents as a centripetal (face and trunk) eruption of pruritic, erythematous, perifollicular papules and pustules. Patients with eosinophilic folliculitis may be subclinically photosensitive. It manifests as discrete erythematous papules, or papules surmounted by a tiny pustule concentrated on the face, neck, upper trunk and proximal part of the upper limbs. It is usually itchy and may be difficult to differentiate from papular pruritic eruption.
Diagnosis: Skin biopsy for EF characteristically shows degranulating eosinophils and mast cells in a perifollicular distribution. Blood tests may be useful in EF as there may be a peripheral eosinophilia.
Treatment: For EF institution of ART is critical. The first line of treatment is topical steroids, emollients, and oral antihistamines. Phototherapy is the most successful treatment modality but other treatments that have been tried including topical disodium cromoglycate, topical tacrolimus, oral antibiotics (erythromycin, tetracyclines, co-trimoxazole), oral itraconazole (for its anti-eosinophilic effect), oral dapsone, oral indomethacin, oral isotretinoin and oral metronidazole with antipruritic agents.
Prevention: The lesions can be reduced by covering the extremities to reduce exposure to insect bites.
Complications: Secondary bacterial infections.




Description: An inflammatory condition that is characterized by chronic and recurrent erythema and greasy scale in areas with terminal hairs and large sebaceous glands. There are two types: infantile and adult types.
Aetiology: The disease is thought to be related to overgrowth or abnormal or exaggerated immune response to Malassezia species (Pityrosporum yeasts). Sebaceous gland secretion, presence of Malassezia yeast, and the host immune response combine to play role in the pathogenesis of this skin condition.
Clinical presentation: Erythema, greasy scale, may also appear as macules or plaques with dry white or crusts or moist oily scale.
Epidemiology: Seborrheic dermatitis is the most common inflammatory dermatoses in HIV-infected children. The infantile type is self-limiting within the first few months of life while the adult type appears around the time of puberty. It affects the scalp, face (nasolabial folds and eyebrows), chest and body folds. The prevalence among HIV-infected individuals is about 40% and as high as 80% among AIDS patients.
Diagnosis: It is a clinical diagnosis, but fungal infection should be excluded with a negative potassium hydroxide test. Histologically, the lesions of seborrheic dermatitis in patients without HIV-1 are those of eczema; however, with chronicity tend to resemble those of psoriasis. Thus, in longstanding cases it may be difficult to differentiate seborrheic dermatitis from psoriasis, both clinically and histologically.
Treatment: Treatment options include topical steroids, antifungals and emollients. The scalp can be treated by washing daily with shampoos containing selenium sulphide, ketoconazole, zinc pyrithione, salicylic acid or coal tar.
Crusts or scales can be removed by overnight application of salicylic acid in water-soluble bases such as aqueous cream. Corticosteroid scalp applications or creams, with or without 2% precipitated sulphur, may alleviate erythema and itching.
For the face, low-potency corticosteroids such as 1% hydrocortisone are usually sufficient. These may be mixed with 2% precipitated sulphur or with an imidazole, as in some proprietary compounds. For the flexures, imidazole and hydrocortisone mixtures are best.
Treatment of the trunk usually requires potent topical corticosteroids. Oral itraconazole, which has activity against Malassezia, may be used at a dose of 100 mg for up to 3 weeks, and may result in long-term remission in some patients. Lithium succinate 5% cream with or without hydrocortisone has been useful in some cases.
Complications: Secondary infection with bacteria (staphylococcus aureus) or viruses (HSV-1).







Description: A chronic skin condition characterized by xerosis, pruritus, and inflammation.
Aetiology: Unclear but "hygiene hypothesis" and the "keratinocyte apoptosis hypothesis" have been proposed. Interactions among genetic, environmental, skin barrier, immune factors, and stress are documented. Symptoms may be exacerbated by allergic reaction to several triggers.
Clinical presentation: Dryness of skin, itch, typical distribution all in a background of positive family history.
Epidemiology: Common among HIV-infected children. The risk of atopic dermatitis was increased by 30% in one study.
Diagnosis: Atopic dermatitis is a clinical diagnosis.
Prevention: There are no specific preventative measures but as in non-infected persons, avoidance of triggers, ensuring that the skin is always well moisturized is helpful.
Treatment: Avoid triggers. Use emollients, steroids and topical immune response modifiers such as tacrolimus.
Complications: Secondary bacterial infections.





Diaper dermatitis (DD) is the most common dermatitis found in infancy. DD was found to be one of the clinical markers of HIV infection in infants in an endemic area. Diaper dermatitis occurs when skin is exposed to prolonged wetness resulting in breakdown of the stratum corneum, the outer protective layer of the skin. Prolonged contact with urine and faeces is associated with irritant diaper dermatitis. Faecal proteases and lipases are the major irritants.
DD causes discomfort and predisposes infants to secondary infection including Candida albicans. It has also been found to be one of the clinical markers of HIV infection in infants in an endemic area.
Irritant contact diaper dermatitis is characterized by patches of erythema and scaling, mainly on the convex surfaces of buttocks, thighs, lower portion of abdomen, pubic region, labia majora, and scrotum
Diagnosis: Diagnosis of primary irritant diaper dermatitis is clinical. Mycological analysis to determine the contamination by Candida is indicated when there is intense erythema, satellite pustules or slow resolution of the disease.
Prevention: The key element of care in irritant contact diaper dermatitis is prevention. Frequent diaper changes are also important in preventing diaper dermatitis.
Treatment: Medical treatment of primary irritant diaper dermatitis consists of simple measures applied according to the severity and type of dermatitis.
Barrier creams made of zinc oxide, titanium dioxide and starch or creams with dexpanthenol may be used to avoid excessive humidity in the diaper area, minimize transepidermal loss of water and reduce skin permeability. These products may help prevent the contact of faeces with the already damaged skin, because they get adhered to the epidermis and are not easily removed with water.
Topical corticosteroids such as hydrocortisone may be applied if erythema persists. If dermatitis does not improve or there is marked erythema and pustules, Candida infection should be suspected and topical antifungals like clotrimazole commenced.




Definition: Psoriasis is a chronic inflammatory skin disease characterized by excessively rapid keratinocyte proliferation.
Epidemiology: The prevalence of psoriasis in HIV-infected persons is the same as in the general population, however the disease is more severe in HIV-infected persons with falling CD4 counts.
Aetiology: Psoriasis has a strong genetic predisposition. In HIV, it is postulated that the immune dysregulation in advanced disease favors development of psoriasis.
Clinical features: Psoriasis in HIV-infected persons has unusual presentations. It is severe and is associated with frequent exacerbations. Several morphological types often coexist in the same patient. The common presentations include plaque, erythrodermic, inverse psoriasis and reactive arthritis-like psoriasis syndrome.
Treatment: Treatment is generally challenging. Initiation of antiretroviral therapy and avoidance of triggers like smoking, beta-blockers and lithium improves response. Topical steroids, vitamin-D derivatives, coal tar and dithranol can be used in mild disease. Acitretin and phototherapy, if available, are recommended in moderate to severe disease. If these fail, under careful supervision, immunosuppressants like methotrexate and cyclosporine may be used.




Introduction: Pityriasis rosea is an acute, self-limiting disease, probably infective in origin, affecting mainly children and young adults, and characterized by a distinctive skin eruption and minimal constitutional symptoms.
Clinical features: Prodromal symptoms are usually absent. The first manifestation of the disease is usually the appearance of the herald patch, which is larger and more conspicuous than the lesions of the later eruption and is usually situated on the thigh or upper arm, the trunk or the neck; rarely it may be on the face, scalp or the penis. It is a sharply defined, erythematous, round or oval plaque, soon covered by fine scale.
The eruption consists of discrete oval lesions, dull pink in colour and covered by fine, dry, silvery-grey scales. The centre tends to clear and assumes a wrinkled, atrophic appearance and a tawny colour, with a marginal collarette of scale attached peripherally, with the free edge of the scale internally. The long axes of the lesions characteristically follow the lines of cleavage parallel to the ribs in a Christmas-tree pattern on the upper chest and back. The skin lesions commonly fade after 3–6 weeks, but some clear in 1 or 2 weeks and a few persist for as long as 3 months.
Treatment: Most cases require no treatment. Symptomatic treatment with antihistamines and topical steroids is often required and in severe cases UVB has sometimes been used. Oral erythromycin and high-dose acyclovir (20mg/kg) five times daily for 1 week), used early after the onset of the eruption, may lead to a more rapid clearance of skin lesions.





Description: This is the dryness of skin and a common cause of pruritus in HIV-infected persons.
Aetiology: Changes in cutaneous micro-circulation and nutrient supply to the skin.
Clinical presentation: dryness of skin, pruritus, excoriations.
Epidemiology: One of the most common non-infectious skin diagnoses in HIV-infected individuals. It is mainly seen in the extremities.
Prevention: Affected individuals should avoid soap and excessive washing.
Treatment: Skin hydration such as soaking in tub (using tepid or lukewarm water) followed by application of emollient. Mid-potency steroids (ointment is better than cream, since it contains lubricant).
Complications: Secondary bacterial infections.

Description: The term ichthyosis is derived from Greek word ‘ichthys’, meaning fish and is basically a heterogeneous group of cutaneous keratinization disorders.
Aetiology: Can be congenital or acquired. Acquired Ichthyosis can be secondary to HIV, sarcoidosis, hypothyroidism and as a paraneoplastic phenomenon. In HIV, it is thought to result from wasting syndrome.
Clinical presentation: There are symmetrical large scales of the skin.
Epidemiology: Acquired Ichthyosis is among the most frequently encountered dermatologic disorders found in HIV-infected persons with advanced disease.
Diagnosis: Xerosis is a clinical diagnosis.
Prevention: Affected individuals should avoid soap
Treatment: ART, skin hydration and lubrication.
