
Description: Herpes simplex viral (HSV) is a common, chronic or recurrent infection in the paediatric HIV population. The clinical presentation of HSV in HIV-infected patients is often atypical and standard therapy often ineffective. HSV infection should be suspected in any chronic vesicular or mucocutaneous ulceration disease and Tzank smear should be performed.
HSV usually affects both the buccal and genital mucosae, but in HIV can affect the skin.
Aetiology:Herpes simplex (HSV) type 1 causes oral lesions while type 2 affects genitalia. An infected mother can transmit the virus to her unborn child through exposure to infected maternal genital fluids.
Clinical presentation: HSV presents as orolabial painful blisters and/or punched out ulcers, which may be associated with fever, irritability and lymphadenopathy. In HIV, the ulcers are chronic and non-healing with rolled edges. A high index of suspicion is needed to make the diagnosis.
In neonates and immune-compromised individuals, it may present as disseminated disease and in this setting encephalitis is not uncommon.
Epidemiology: In any population and age group, HSV-1 is more common than HSV-2 and the prevalence of HSV-1 in non–high-risk populations increases in a linear fashion with age, with most initial infections occurring in childhood and adolescence. HSV-1 prevalence is > 40% in 15 year olds, before increasing to 60%–90% in adulthood. HSV-2 is prevalence is strongly associated with age, increasing from negligible levels in children <12 years to as high as 80% amongst older higher risk populations.
Diagnosis: In uncomplicated cases, the diagnosis is mainly clinical, but a Tzanck smear, viral culture, PCR technique is helpful in atypical cases including CSF PCR or culture in suspected encephalitis.
Prevention: HSV is transmitted most commonly during delivery, but also can be transmitted in utero or through postnatal contact with the mother or other caretakers. Prevention is therefore crucial, some specialists recommend prophylactic acyclovir therapy, some recommend routine caesarean section and others recommend both. However, for those who have a history of recurrent genital HSV, a recent review of best evidence found insufficient data to support the use of prophylactic acyclovir. Contact with infected vesicles should be avoided.
Treatment: The drug of choice for treating localised HSV infection in infants and children is acyclovir. The recommended dose is 20 mg/kg/day in five divided doses Xu-10 days. Usually if the child <2 years: acyclovir 100 mg 5 times a day for 10 days or 200 mg three times a day for 10 days.
If child >2 years: acyclovir 200mg 5 times a day for 10 days or 400 mg three times a day for 10 days. In case of acyclovir resistance or where available: Foscarnet 120-200 mg in two to three divided doses can be used.
Although commonly prescribed by many physicians, topical antiviral medications such as acyclovir ointment are not recommended to treat most mucocutaneous HSV lesions because such therapy does not reduce the severity or duration of infections in immunocompetent hosts. Topical therapy can be used in immunocompromised patients to accelerate the healing of lesions.
Complications: Dissemination, concomitant infection with other pathogens including viruses, such as CMV, yeasts infection (Candida) or secondary bacteria may occur. Potential risk of developing HPV associated epithelial neoplasia exists.





Patients with atopic dermatitis are susceptible to acute generalised infections with herpes simplex virus, referred to as eczema herpeticum. Eczema herpeticum can be caused by either type 1 or type 2 HSV. Eczema herpeticum in immunocompromised children such as those who have HIV, tend to have higher risks of dissemination and longer durations of outbreaks and are less responsive to therapy.
Description: Folliculitis is the inflammation of the hair follicle. It can be caused by physical injury, chemical irritation or an infection.
Aetiology: Staphylococcus aureus is the most frequent cause of infective folliculitis but folliculitis can also be caused by pathogenic fungi e.g. Candida albicans, commensal fungi such as Malassezia furfur and mites such as Demodex species. These are most often seen on the face in immunosuppressed children.
Clinical presentation: The presentation may be in the form of itchy, painless or painful papules, dome-shaped pustules (with hair shaft at the centre) often with an erythematous base. Folliculitis has predilection for the scalp, extremities, occluded areas and areas prone to excessive moisture and chafing. Systemic symptoms are not common.
Eczema herpeticum presents as monomorphic eruptions of dome-shaped vesicles that may transform into pustules. The vesicles dry out within 2 to 3 weeks and may leave erosive pits. These "punched out" erosions can create a scalloped appearance at the periphery of the large denuded area.
Eczema herpeticum is a clinical diagnosis and can be confirmed by a Tzanck smear, performed by unroofing a vesicle and scraping the base of a lesion. On light microscopic examination, multinucleated giant cells are seen. HSV culture, PCR or a direct fluorescent antibody test are other confirmatory tests. When a secondary infection is suspected, a bacterial culture is obtained.
Prevention: Parents of children with moderate to severe eczema should be made aware of eczema herpeticum and advised to seek help early. Children with atopic eczema, especially those with a history of eczema herpeticum, should avoid close contact with relatives and friends with active herpes simplex.
Secondary bacterial infection with S aureus or ß-haemolytic streptococci may occur which may be indicated by yellow crusting. The secondary infection may be heralded by a high fever and other systemic symptoms. A more severe complication is periorbital eczema herpeticum that can result in keratoconjunctivitis with possible stromal scarring and subsequent blindness. Patients who have eye involvement require immediate ophthalmologic evaluation.
Treatment: Severe cases require acyclovir, as early as possible for 7 days and oral antibiotics if secondary bacterial infection is suspected. The underlying eczema should be treated to avoid recurrences. EH is not necessarily more common in HIV, but needs higher and longer doses of treatment.



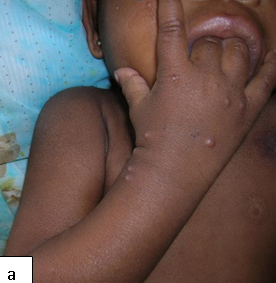
Herpes zoster is rare in immunocompetent children but an increased incidence is described in HIV- infected persons, sometimes as an early clinical sign of the development of AIDS.
Description:t is usually localized to a dermatome as a result of reactivation of the dormant virus in the sensory ganglion acquired during primary varicella or chicken pox infection. The word zoster means a girdle because it passes round the body like a girdle.
Aetiology:Is caused by a neurodermotropic virus called varicella zoster virus. It follows a clinical or sub clinical varicella (chicken pox) infection early in life or occasionally in utero. Predisposing factors include HIV infection, chronic steroid use, malignancies and diabetes mellitus.
Clinical presentation:The prodromal symptoms are hyperesthesia, paresthesias, burning dysesthesias or pruritus along the affected dermatome(s). The most common presenting features are pain and vesiculations Thoracic and cranial nerves are the most commonly involved. In most situations herpes zoster is confined to a single dermatome but can be multidermatomal or disseminated in HIV- infected children.
Epidemiology:It is distributed worldwide and is a common complication of HIV.
Diagnosis:Diagnosis is mainly clinical but in cases of uncertainty, Tzanck smear, viral culture, PCR is helpful.
Prevention:Varicella zoster vaccine in susceptible individuals.
Treatment: Rest and analgesics are sufficient for mild attacks of zoster in the young. Soothing antiseptic applications may be helpful and secondary bacterial infections require antibiotics. Treatment of HZ is with antivirals: acyclovir 200mg five times a day for 7 days or IV acyclovir 5 mg/kg 8-hourly. In case of acyclovir resistance: Where available: Famciclovir and valacyclovir are other options. Foscarnet 120-200 mg in two to three divided doses, in case of acyclovir resistance or when available. The antiviral medications are most effective when started within 72 hours of onset of the rash. Opioids, tricyclic anti-depressants and anti-convulsants are useful in managing post-herpetic neuralgia.
Complications: Post-herpetic neuralgia, secondary bacterial infections. Recently, a vaccine has been developed for varicella zoster, which should reduce the population frequency of post-herpetic neuralgia. Encephalitis other main systemic complications are varicella pneumonia and hepatitis.



The different morphological variants of warts are found in 5-30% of patients with HIV infection.
Description: These are flat warts (verruca plana).
Aetiology:Human papilloma virus (HPV) type 3 and, less often, types 10, 27, and 41 are the causative agents of verruca plana.
Clinical presentation: The warts are very slightly elevated above the level of surrounding skin and can be slightly hypo or hyperpigmented. Plane warts in HIV infection tend to be extensive and may be photodistributed.
Epidemiology: Plane warts are common and have no gender predilection. Prevalence of about 20% in HIV-infected children has been reported. Transmission can be either directly through person to person contact or indirectly through sharing of fomites.
Diagnosis: Diagnosis is mainly clinical. In cases of doubt PCR and histology are helpful.
Prevention: Healthy skin care and avoiding skin contact with an infected person.
Treatment: Response to treatment is usually unsatisfactory. Treatment options include salicylic or lactic acid in flexible colloidal preparations and 0.05% tretinoin creams. Initiation of ART does not seem to improve plane warts.
Complications: Potential risk of development of HPV associated epithelial neoplasia
Description: Epidermodysplasia verruciformis (EV) is an inherited clinical variant of verruca plana in which there is widespread and persistent infection with HPV. Patients frequently harbor multiple HPV subtypes. Subtypes 5 and 8 are associated with squamous cell carcinomas. The other subtypes are 14, 17, 20 and 47.
Clinical presentation: A characteristic combination of plane warts, pityriasis versicolor-like lesions and reddish plaques.
Complications:Malignant transformation occurs in 20 - 40% of patients and onset is usually in the 20s. However metastatic disease is rare.
Prevention:Avoidance of excessive sun exposure, with diligent use of effective sunscreen.
Treatment:Patients should be observed for the development of squamous cell carcinomas and premalignant lesions, which should be excised or locally ablated. Oral retinoids have been used but their long-term effectiveness is uncertain.
First-line option: etretinate, starting dose of 1 mg/kg/day, but the effect is dose dependent and relapse occurs if the drug is stopped.
Second-line option: The combination of etretinate plus IFN-α may also produce a useful clinical effect.
Other options include oral isotretinoin, which has been shown to improve the clinical appearance of the benign lesions. Occasional but inconsistent benefits have been reported with topical imiquimod, topical vitamin D analogues, topical immunotherapy with squaric acid dibutylester and oral cimetidine.



Clinical Presentations:Verrucous papules on palms and soles. Common warts can be verrucous, mosaic or filiform. Periungual involvement common.
Epidemiology: HIV-infected children are more susceptible and the warts tend to be more extensive and recalcitrant
Diagnosis:The diagnosis is based upon clinical appearance. Paring of overlying hyperkeratotic debris usually reveals thrombosed capillaries. This helps to differentiate warts from calluses. In cases of doubt PCR and histology are helpful.
Prevention: Advice on simple measures to limit the spread of the infection by avoiding physical contact with the warts and cleaning of fomites may be advised.
Treatment: Treatment options include salicylic acid, cantharidin, topical 5-fluorouracil, cryotherapy, paring, cautery or CO2 laser.



Clinical Presentation: Whitish or pale papules with a smooth or roughened surface. Can affect any part of the oral cavity.
Epidemiology: HIV-infected children are more susceptible to oral warts, which are rare in immunocompetent persons. In the era of ART, the prevalence of oral warts is increasing estimated to be between 1.6 – 2.6%.
Diagnosis: Diagnosis is mainly clinical. In cases of doubt PCR and histology are helpful. Human papilloma virus types 13 and 32 are the most commonly implicated.
Prevention: Avoid biting warts in other areas of the body.
Treatment: Treatment options include surgery, cautery or CO2 laser. Topical imiquimod 5% cream has been successfully used.Complications: Potential risk of development of HPV associated epithelial neoplasia.

Description: Warts on the genital and perianal area have variable clinical presentations.
Aetiology: At least 40 subtypes of human papilloma virus (HPV) have been shown to cause genital warts. Of these subtypes 16 and 18 are considered to be high risk as they are associated with development of squamous cell carcinomas.
Clinical presentation: anogenital warts (condylomata acuminata) may present as flat, dome-shaped, cauliflower-shaped, or pedunculated lesions.
Epidemiology: Anogenital warts are common sexually transmitted disease estimated to occur in 1% of sexually active adults. In young children, they may be an indication of sexual abuse.
Diagnosis: Diagnosis of anogenital warts is mainly clinical and the diagnosis can be confirmed by histology or PCR. The latter is used for subtyping to rule out high risk subtypes.
Prevention: Advice on simple measures to limit the spread of the infection by avoiding physical contact with the warts and cleaning of fomites may be advised. HPV vaccines are effective for prevention of HPV-associated malignancies.
Treatment: Not all warts need treatment as many give little inconvenience and will resolve spontaneously. Where treatment is needed first-line options include 20% podophyllin, cryotherapy and salicylic acid. Second-line options include imiquimod. Spontaneous remission has been reported in 20-30 of infected patients.
Complications: Potential risk of developing HPV associated epithelial neoplasia exists. Genital warts in children may be a manifestation of child abuse.




Description: A contagious disease caused by measles virus with characteristic rash that starts from the face and spreads to the extremities.
Aetiology: Measles is caused by the measles virus. Lack of immunization is a risk factor although disease has been recorded among immunized infants. Vitamin A deficiency state has been associated with severe disease.
Clinical presentation: High grade fever is usually the first sign of measles at about 10 to 12 days after exposure to the virus, and lasts four to seven days. Other symptoms in the initial stage are catarrh, cough, red and watery eyes, and small white spots inside the cheeks (Koplik’s spots). Koplik’s spots are pathognomonic for measles but last for less than 24 hours. A maculopapular rash follows, usually on the face and upper neck after several days and then spreads to reach the hands and feet. The rash lasts for five to six days, and then fades. On average, the rash occurs 14 days after exposure to the virus (range 7 – 18 days).
Epidemiology: The incidence in Africa is estimated to be as high as 17. 2 cases per 100,000 population. There is a higher incidence of contracting measles in HIV-infected children. In addition, there is an increased case fatality. Outbreaks of the disease still occur in parts of Africa. The virus is spread by close contact with infected nasal or throat secretions.
Diagnosis: Detailed history, including immunization history and a thorough physical examination for characteristic features should be done. Demonstration of measles IgM antibodies (where available) confirms the diagnosis.
Prevention: Routine measles vaccination for children (at 9 months of age) combined with mass immunization campaigns in countries with high case and death rates. The World Health Organization recommends two vaccinations at 6 and 9 months for HIV exposed and infected children. The vaccine is safe, effective and inexpensive. It may be given in combination with rubella and/or mumps vaccines in countries where these illnesses are problems. It is equally effective in the single or combined form.
Treatment: There is no effective anti-viral treatment. Supportive care is the mainstay and should ensure good nutrition, adequate fluid intake and treatment of dehydration. Antibiotics should be prescribed to treat secondary pneumonia and bacterial infections of the eye and ear. Two doses of vitamin A supplements, given 24 hours apart is recommended for all children diagnosed with measles in developing countries. Vitamin A supplements have been shown to reduce the number of deaths from measles by 50%.
Complications: Blindness, encephalitis, diarrhoea, otitis media, lower respiratory infections such as pneumonia




Description: Molluscum contagiosum (MC) is a common viral skin infection of the skin.
Aetiology: MC is caused by poxvirus – a DNA virus from the Poxviridae family.
Clinical presentation: Usually present as small pearly, dome shaped, small, discrete lesions with central umbilication. In HIV-infected individuals, atypical varieties such as large or non-umbilicated lesions are found. Individual papules may coalesce to form the agminate variety. Lesions tend to be recalcitrant and resistant to treatment.
Epidemiology: MC is seen in 10-20% of AIDS patients. Transmission is by autoinoculation and physical contact.
Diagnosis: mainly a clinical diagnosis but a skin biopsy staining of the curdy material with Giemsa and demonstration of eosinophilic molluscum bodies can be helpful in atypical cases.
Prevention: Avoidance of close contact with infected persons.
Treatment: Infection is usually self-limiting and spontaneously resolves after 18-24 months in mild cases and therefore no treatment may be necessary. If problematic and extensive the most commonly used therapeutic options include 5% salicylic acid/lactic acid preparations, trichloroacetic acid, curettage, cautery and cryotherapy. Less commonly imiquimod cream, tretinoin cream, cantharidin and benzyl peroxide are used with variable success. Large lesions can be removed surgically. Treatments may cause scarring and leave marks long term. HAART improves outcome in HIV-infected children and should be considered in eligible patients.
Complications: Infected and inflamed MC can cause disfigurement and scarring.






| Infection | First-line treatment | Alternative treatment | Where available |
|---|---|---|---|
| HSV | Acyclovir | Valacyclovir Famciclovir | Foscarnet |
| Eczema Herpeticum | Acyclovir | Valacyclovir Famciclovir | Foscarnet |
| Herpes Zoster | Acyclovir | Valacyclovir Famciclovir | Foscarnet |
| Verruca Plana | Salicylic/lactic acid | 0.05% tretinoin creams | |
| EDV | Oral cimetidine | Isotretinoin etretinate plus IFN-α | Imiquimod Vitamin D analogue Squaric acid dibutylester |
| Genital Warts | 20% Podophyllin | Imiquimod | |
| Molluscum contagiosum | 5% salicylic Acid/lactic acid benzoyl benzoate | Trichloroacetic acid Liquid nitrogen Tretinoin cream |
Curettage Cautery Imiquimod cream Cantharadin |
| Measles | Vitamin A supplements | Antibiotics as required |
EDV- Epidermodysplasia verruciformis