
Description: Dermatophyte infections are common in HIV-infected children. They include: tinea capitis, tinea corporis, tinea unguium and tinea pedis.
TineaAetiology: These infections are caused by fungi called dermatophytes, which produce an enzyme called keratinase to break down keratin.
Clinical presentation: Depends on part of the body affected. In the skin, it presents as “rings” (ring worm), with raised edges and clearing at the centre of the lesions, alopecia in the scalp (tinea capitis), may present with scaly feet and/or macerated web spaces (tinea pedis) or may involve the nails leading to the destruction and discoloration of the nails (tinea unguium).
Epidemiology: Common around the world. Specific fungal aetiology varies from one geographical region to another.
Diagnosis: Is mainly clinical but a simple potassium hydroxide (KOH) preparation may be helpful. A KOH mount can be easily prepared by gently scraping the infected skin or blister roof with a sterile scalpel blade onto a glass slide with 1 to 2 drops of 10% KOH. The sample is then examined under the microscope for the presence of hyphae. Alternatively, specimen can be sent for fungal culture for identification of the causative organism and Under Wood’s lamp (UV) colonies will fluoresce.
Prevention: Changing footwear frequently, drying feet well after bathing (especially between toes), refraining from sharing articles of clothing, and appropriately treating friends and family members of affected patients, can be very helpful in minimizing risks of exposure and reinfection.
Treatment: The treatment of dermatophyte infections usually involves the use of oral terbinafine, fluconazole, itraconazole, griseofulvin or one of several well-tried topical preparations.
A commonly used oral antifungal of choice is griseofulvin 10-20 mg/kg for at least 6 weeks for skin and hair infection, 6 weeks for tinea capitis and in severe hair, skin and scalp infections, up to 3 months.
Generally, topical therapies are used for localized or mild infections, oral antifungals for the more extensive infections. There is a variety of topical antifungal agents, including clotrimazole, econazole, oxiconazole, miconazole, terbinafine, and naftifine applied to the affected areas twice daily for 2 to 4 weeks.
For nail infections, longer therapy with oral agents is usually necessary. However, children respond better to topical therapy than adults because of a thinner nail plate and potentially faster nail growth rate.
Complications: Secondary bacterial infection and ID reaction (autoeczematisation as a hypersensitivity reaction to the fungus).












Tinea infections results in diverse clinical features, ranging from the carrier-state to severe tinea corporis with heavy inflammation.
Although the clinical features of tinea may be similar to those seen in adults with erythema and scaling, signs of dermatophyte infection in children may be nonspecific and mimic other conditions, such as psoriasis, atopic dermatitis, contact dermatitis, dyshidrotic eczema, juvenile plantar dermatosis, impetigo, herpetic infection, and cellulitis. Vesicles and bullae may also be more common in children with inflammatory tinea, mimicking bacterial or herpetic cellulitis.

Description: A mild, chronic infection of the skin caused by Malassezia yeast.
Aetiology: Is caused by the fungi Malassezia and the infection is milder and more superficial than the dermatophyte infections. Isolated species of Malassezia in patients include M. globosa, M. sympodialis, M. furfur, M. obtusa, and M. restricta.
Clinical presentation: The primary lesion is a sharply demarcated macule, sometimes slightly erythematous, but characterized essentially by fine, discrete or confluent branny scale that can be hyperpigmented or hypopigmented mainly on the upper trunk. The scale can be accentuated by stretching the lesions, making them scalier.
Epidemiology: Affects adolescents and adults. Prevalence of tinea versicolor is as high as 40% has been reported in the tropics. Climatic and local environmental factors account for variation in the prevalence seen in different geographical regions.
Diagnosis: This is mainly clinical but potassium hydroxide direct microscopy or visualization of the scaly lesions under Wood’s lamp (UV), which shows the typical yellow fluorescence.
Differential diagnoses: Vitiligo and chloasma are normally distinguishable by their complete absence of scaling. Differential diagnoses include: seborrheic dermatitis, pityriasis rosea, secondary syphilis, pinta and tinea corporis.
Treatment: Selenium sulphide in a detergent base, available as shampoo or lotion in 1% or 2.5% concentrations (Selsun® shampoo Blue, Head & shoulders), applied to all the affected areas and left for 10 minutes before washing off or left overnight. In ordinary cases that settle spontaneously or as a result of treatment, the residual depigmentation may remain for many months without any scaling.
Other options include the topical azole antifungals (clotrimazole and ketoconazole). Terbinafine 1% cream is also effective. For widespread lesions topical ketoconazole, 2-3 applications may suffice.
For prophylaxis, selenium sulphide may be applied overnight once a month. Alternatives include 20% sodium hyposulphite solution, and 50:50 propylene glycol in water used long-term as suppressive therapy to prevent relapse.
Oral ketoconazole and itraconazole are also very effective especially when combined with topical antimycotics. Ketoconazole is not recommended in children <10 years. Fluconazole as a single 6 mg/kg dose may also be adequate but some patients may require longer periods of therapy. Itraconazole is active against pityriasis versicolor in a dose of 5 mg/kg usually given over 5 days.
Complications: In ordinary cases that settle spontaneously or as a result of treatment, the residual depigmentation may remain for many months without any scaling. Disfigurement of the affected areas and deep invasive infections may occur in untreated cases.



Description: Candidiasis is the most common opportunistic infection seen in HIV-infected children. It can affect the oral cavity, the oesophagus and the peri-anal region.
Aetiology: Candida albicans is the yeast responsible or candidiasis.
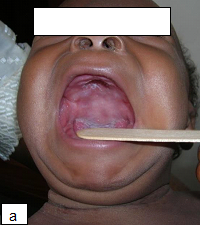
Clinical presentation: Oral candidiasis (thrush) occurs on the surface of the tongue, palate and buccal mucosa as white patches (plaques). This can be distinguished from milk curds by scraping the surface of the plaque, which results in erythema and point bleeds.Pseudomembranous candidiasis manifests as creamy white-to-yellow oral plaques. Atrophic candidiasis manifests as distinct areas of erythema with the loss of tongue papillae if the tongue is affected. Hyperplastic candidiasis (with both erythematous and white mucosal coloration symmetrically distributed) and angular cheilitis are other clinical variants of candidiasis.
Oral thrush can be seen in neonates and in patients receiving prolonged antibiotics and systemic steroids. Oesophageal candidiasis presents with dysphagia, odynophagia and retrosternal pain. Diaper rash due to candidiasis is usually red with a clearly defined border and consists of small red spots close to the large patches (satellite lesion). Diaper rash lasting for 3 days or longer may be candidiasis. Candida albicans is one of the causes of onychomycosis. In severely immunocompromised children the organism can cause candidemia or invasive candidiasis.
Epidemiology: Candida albicans is the most common cause of mucosal and oesophageal candidiasis. Oral thrush and diaper dermatitis occur among 50%-85% of HIV-infected children.
Diagnosis: Candidiasis is a clinical diagnosis which can be confirmed by a potassium hydroxide preparation and culture. Cobblestoning appearance on barium swallow may be seen in oesophageal candidiasis.
Prevention: In the mouth, for instance, this involves frequent toilet in the seriously ill, and denture hygiene in other patients, whereas in Candida infections affecting the skin, careful drying of affected sites is important.
Treatment: In many cases, topical antifungal therapy alone is sufficient to control the disease. Effective topicals include clotrimazole, nystatin and amphotericin B. Systemic therapy with fluconazole, itraconazole or amphotericin B is indicated in oesophageal disease. In addition, oral antifungals are used to prevent systemic candidiasis in severely immunocompromised patients. Clotrimazole troches or lozenges are used at 50mg 5 times a day while fluconazole and itraconazole dosing are 3-12mg/kg/day and 5mg/kg/day respectively.
Children with severe oral involvement due to diffuse and persistent candidiasis resistant to conventional treatment also tend to have feeding difficulties that may be related to oesophageal involvement. In these cases, the only effective therapy is intravenous fluconazole or amphotericin B.
Complications: Haematogenous dissemination of disease and invasive candidiasis can occur, resulting in candidemia, meningitis, endocarditis, renal disease, endophthalmitis, and hepatosplenic disease.



C. albicans is commonly isolated from the moist skin of the buttocks and genitalia of the infant but is more prevalent where the skin is affected by napkin rash. Satellite lesions may be seen.
Diagnosis: moistened swab or a scraping may be taken to discover whether or not Candida is present on the affected skin. If Candida is present, a trial of anti-candida therapy is indicated.

Description:
Aetiology: Histoplasmosis is a fungal infection caused by the dimorphic fungus Histoplasma capsulatum.
Clinical presentation: Histoplasmosis is mainly inhaled and usually presents as a disseminated disease. Localized infections are rare. Skin may be the most frequent site of localised infection.
The cutaneous lesions of histoplasmosis are polymorphous and include papules, plaques, which may be crusted, erosions, ulcers, exanthems, nodules, acneiform eruptions, exanthems, molluscum-like lesions, acneiform folliculitis, psoriasiform eruptions, panniculitis, hyperkeratotic plaques, vasculitic lesions, erythema multiforme-like lesions, exfoliative dermatitis, abscesses and cellulitis. Oral ulcers and erosions are the most common manifestation of disseminated disease. There may be associated systemic symptoms including fever, lymphadenopathy, hepatosplenomegaly, lung disease and pancytopenia.
Diagnosis: Chest X-rays, tissue biopsies for histology and culture aid diagnosis. Histoplasma capsulatum can be identified on skin biopsy by the Gomori methenamine silver stain however culture of the organism is the gold standard.
Treatment: In addition to ART, infected patients benefit from systemic antifungal treatment with itraconazole or amphotericin B with long-term prophylaxis. For disseminated infection, the preferred approach is to give IV amphotericin for 4 weeks followed by itraconazole prophylaxis.



Figures 52 – 54 above emphasize the polymorphous nature of histoplasmosis lesion.
Aetiology: Cryptococcosis is caused by Cryptococcus neoformans.
Clinical presentation: Brain, lung and skin are sites of predilection. In the skin, it presents as jelly-like necrotizing papules and nodules that resemble molluscum contagiosum. Acneiform, tumourous (warty) and papulopustular variants of the disease have been documented.
Epidemiology: Before the advent of ART, was estimated to affect 5-10% of persons with AIDS in the US and UK, and 30-40% in Africa.
Diagnosis: For systemic disease, serology, blood culture, urine culture and lumber culture should be done. Cutaneous disease can be confirmed by skin biopsy with special stains for the cryptococcal capsule and culture or Tzanck smear.
Treatment: Intravenous amphotericin B and oral fluconazole (see cryptoccocal infection in Part 2 of the atlas). Secondary prophylaxis is with fluconazole.


A recent report of cases of a new species of dimorphic fungus pathogenic to humans, especially in human immunodeficiency virus-infected was made in South Africa adults, most of whom presented with lung and skin lesions. A case of disseminated emmonsiosis has also been reported in an HIV-infected child. The child had severe immunosuppression (CD4+ T cell count 0.012 x 109/L). The DNA sequence was identical to the disseminated disease caused by the novel organism. Many of these cases of emergomycosis had initially been diagnosed as histoplasmosis.
Aetiology: Causative organism: closely related to Emmonsia pasteuriana now called Emergomyces africanus.
Treatment: Amphotericin B given for 6 weeks, in addition to initiation of ART.
Background: A deep fungal infections more common in adults affected with HIV than children. In immunocompetent individuals, infection generally results from cutaneous inoculation by trauma it may present as a disease of the skin and draining lymphatics. Sporotrichosis associated with HIV may in addition occur as pulmonary infection following spore inhalation and may be haematogenously spread from pulmonary infection to the skin and joints.
Aetiology: The agent, Sporothrix schenckii, a dimorphic fungus found in soil and in animal faeces, is responsible for most infections.
Epidemiology: Sporotrichosis is relatively uncommon even though it shares a worldwide distribution. In some parts of the world, the condition follows cat scratch or contact with the affected animal’s wound.
Diagnosis: Tissue biopsy and fungal culture are the mainstay of diagnosis. Blood culture samples, bronchoalveolar lavage or CSF for microscopic examination may be helpful.
Clinical: On the skin, sporotrichosis presents as suppurating nodules that progress onto ulcers at the point of inoculation and progress proximally along lymphatic vessels. In disseminated disease the skin lesions are widespread.
Other organs can be affected in visceral disease including the CNS, joints, spleen, bone marrow, pneumonia, meningitis and eyes.
Treatment: Amphotericin B at a dose of 0.7mg/kg per day for 3 to 4 weeks. Potassium iodide, normally used for infected patients is not recommended for HIV/AIDS patients. Other options include itraconazole and fluconazole.

| Condition | First line | Second line | Where available/ indicated |
|---|---|---|---|
| Superficial fungal infections | |||
| Tinea Corporis | Topical agents: including clotrimazole, econazole, oxiconazole, miconazole, terbinafine, naftifine |
Oral griseofulvin | Terbinafine, itraconazole, fluconazole |
| Tinea Capitis | Oral Griseofulvin 10mg/kg daily x 6 weeks | Fluconazole- 6mg/kg once weekly for 6 weeks | Oral terbinafine, itraconazole |
| Candidiasis | Topical clotrimazole, nystatin | Clotrimazole troches | Severe infection - systemic agents: fluconazole, itraconazole, amphotericin B |
| Pityriasis versicolor | Topical clotrimazole, nystatin | Ketoconazole shampoo, terbinafine 1% cream | Oral ketoconazole, itraconazole |
| Deep fungal infections | |||
| Histoplasmosis | Oral itraconazole | Amphotericin B | |
| Cryptococcosis | Amphotericin B + Fluconazole | Fluconazole only | |
| Sporotrichosis | Amphotericin B | Itraconazole | Fluconazole |