Parotid enlargement is estimated to occur in about 3 to 6% of HIV positive adults and 1 to 10% of children and is so unusual in the HIV negative population that cystic enlargement of the parotid gland is an indication for HIV testing. It is secondary to benign lymphoepithelial cysts and is categorised under stage 2 HIV disease
Diagnosis: Differential causes of swellings in and around the parotid region in paediatric age group include viral infections such as mumps (epidemic parotitis), Ebstein-Barr virus and HIV. The parotid enlargement tends to be bilateral in viral causes of parotitis but may be unilateral. Acute bacterial parotitis from Staphylococcus aureus and anaerobes found normally in the mouth generally cause a unilateral swelling and other symptoms such as pain and fever may be present. Tuberculosis and malignancies such as lymphoma are also important differentials.
In HIV parotitis, fine needle aspiration cytology (FNAC) may show background generalized marked lymphocytosis and occasional macrophages. Some cases may show cellular aggregates suggestive of epithelial components.
Treatment:The swelling is managed conservatively with antiretroviral therapy. In one study, there was marked reduction in parotid enlargement and significant improvement in CD4 count, CD4 % and viral load following the commencement of ART in majority of the cases. Sclerosing therapy, external beam RT and surgery are other reported treatment options.
Further reading
Adedigba M, Ogunbodede E, Jeboda S, et al. Patterns of oral manifestations of HIV/AIDS among 225 Nigerian patients. Oral Dis 2008; 14(4):341–6.
Dave S, Pernas F, Roy S. The benign lymphoepithelial cyst and a classification system for lymphocytic parotid gland enlargement in the pediatric HIV population. Laryngoscope 2007; 117(1):106–13.
Schrot R, Adelman H, Linden C, et al. Cystic parotid gland enlargement in HIV disease: the diffuse infiltrative lymphocytosis syndrome. JAMA 1997;278:166–7.
Favia G, Capodiferro S, Scivetti M, et al. Multiple parotid lymphoepithelial cysts in patients with HIV infection: report of two cases. Oral Dis 2004; 10:151–4.
Huang R, Pearlman S, Friedman W, et al. Benign cystic vs. solid lesions of the parotid gland in HIV patients. Head Neck 1991; 3: 522–7.
Mandel L, Surattanont F. Regression of HIV parotid swellings after antiviral therapy: case reports with computed tomographic scan evidence. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94: 454-9.
Morales-Aguirre JJ, Patino-Nino AP, Mendoza-Azpiri M, et al. Parotid cysts in children infected with human immunodeficiency virus. Arch Otolaryngol Head Neck Surg 2005; 131: 353–355.
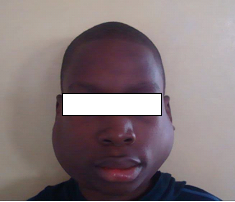
Figure 95: Bilateral parotid enlargement in a 4-year-old child erroneously
diagnosed as a case of mumps. More detailed history, examination and
antibody testing confirmed HIV infection.Figure 96: Bilateral parotid swelling in a 12-year-old child.