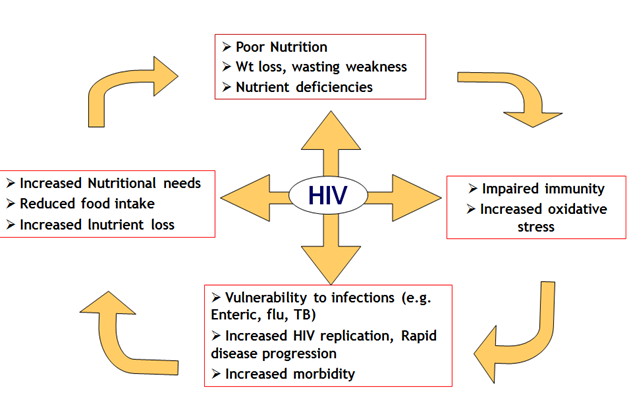
Figure 100: Interaction between HIV infection and nutritional status in children
Malnutrition is high among HIV-infected children especially in developing
countries, where it is already endemic. Severe malnutrition is predictive of
HIV; 30—50% of severely malnourished children are HIV-infected in settings
where both conditions are endemic.
Stunting (low height for age) is a more prominent feature than wasting in HIV associated
malnutrition. Micronutrient deficiencies (low serum levels of zinc,
selenium, vitamins A, E, B6, B12 and C) is also common among HIV-infected
children. HIV-related malnutrition could result from reduced food intake (poor
appetite, oral infections such as candidiasis), increased metabolism and poor
absorption of nutrients mainly due to diarrhoeal diseases.
Unexplained moderate malnutrition not adequately responding to standard
therapy is classified as stage 3 disease. Unexplained severe wasting, stunting
or severe malnutrition not responding to standard therapy is a clinical stage 4
disease.
Diagnosis
Weight, height and occipitofrontal circumference (OFC) should be
plotted on available growth charts (WHO growth standards available at
www.who.int/childgrowth/training/en).
- SD Z scores for weight, height/length, OFC (from -2SD to -3SD is
severe)
Severe wasting can also be demonstrated by measuring the mid
upper arm circumference (MUAC):
< 11.5 cm from 6 - 59 months of age:
< 13.5 cm from 5-9 years
< 16.0 cm from 10-14 years
Treatment
It is recommended that children with severe acute malnutrition (SAM) are
managed in the institution until there is nutritional recovery, ≥90% weight for
height. Generally, this would require admission for up to 4 weeks.
Children can be discharged once they have achieved >10 g/day weight gain,
are taking a solid diet, have a good appetite, show no oedema.
Ready to use foods (RTUF) e.g. plump nuts, a new peanut butter based F100
preparation is useful as therapeutic and supplemental feed in the
management of severe malnutrition.
Complications
Mortality is five times higher in severely malnourished HIV-infected than in
uninfected children.
Further readings:
WHO. Antiretroviral Therapy for HIV infection in children and infants:
Toward Universal Access. Recommendations for a public health approach.
2010 revision. Available from:
http://whqlibdoc.who.int/publications/2010/9789241599801_eng.pdf.
Duggal S, Chugh TS, Duggal AS. HIV and Malnutrition: Effects on Immune
System. Clinical and Developmental Immunology 2012; 1-8.
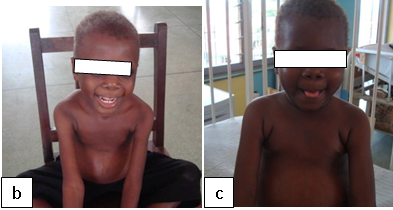
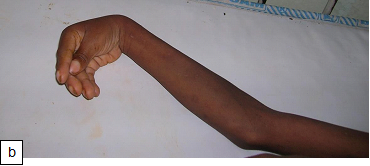
Figure 101: Plump NutsFigure 102:Severe malnutrition: MUAC 10.5 cm. Figure 103a: Severe wasting Figure 103b: Marasmus with gluteal skin folds (“baggy pants” sign).Figure 104: Severe wasting with hair changes in HIV infection.Figure 105a: At first diagnosisFigure 105b & c: (b) After 2 weeks on care (c) After 4 weeks on care.Figure 106a & b: Severe wasting and flaky paint desquamation on the lower limbs of an HIV-infected child.Figure 107a & b: 8-year-old boy with severe acute malnutrition plus oedema. He had symptomatic hypocalcaemia with carpal spasm demonstrated. The spasm resolved with intravenous calcium gluconate.Figure 108:Angular stomatitis due to riboflavin (vitamin B2) deficiency.