LIP is a slowly progressive interstitial lung disease seen in HIV-infected children. LIP is rare in non-HIV-infected children and in HIV-infected adults. The usual age of presentation is older than 2 years of age. The pathogenesis is thought to be due to primary infection with Epstein-Barr virus, which initiates a lymphoproliferative response from co-infection with HIV.
Clinical presentation: Children with LIP usually present with chronic respiratory symptoms of cough and slowly progressive hypoxia, tachypnoea, exertion fatigue and reduced oxygen saturation. There may be an acute-on-chronic presentation with fever and tachypnoea, when there is superimposed bacterial pneumonia. Apart from the lungs, there is also lymphoproliferation in other organs, hence LIP may be associated with bilateral non-tender parotid enlargement, persistent generalised and symmetrical lymphadenopathy, hepatosplenomegaly, and/or adenoidal and tonsillar hypertrophy. Digital clubbing is commonly associated with LIP.
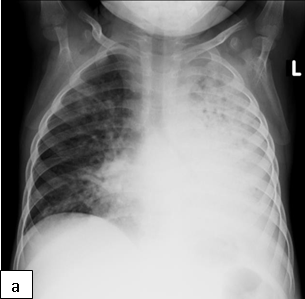
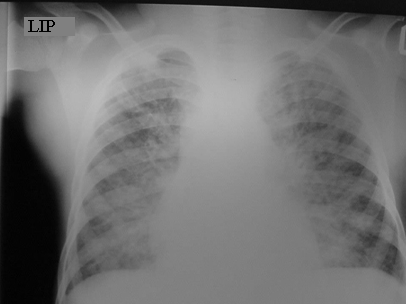
Characteristic chest radiographic findings of LIP include bilateral, diffuse, reticulonodular infiltrates that are more prominent in the lower lobes, and bilateral hilar adenopathy. Distinguishing LIP from PTB or miliary TB can be a challenge.
Differential diagnoses: Bacterial pneumonia, PCP, Tuberculosis, CMV pneumonitis, other viral pneumonia, e.g., RSV, influenza, parainfluenza, adenovirus; malignancy, e.g., Kaposi sarcoma, lymphoma, fungal pneumonia, MAC infection and nocardiosis.
Treatment: Institution of ART is necessary. Additionally, oral prednisone 2 mg/kg/day for 2–4 weeks followed by reduced dosage are indicated in children with dyspnoea and hypoxia. Additional treatment with antibiotics may be required when secondary bacterial infection is suspected.

Bronchiectasis is defined as an abnormal dilatation of airways. Recurrent or persistent lung disease associated with HIV e.g. recurrent or unresolved bacterial pneumonia, LIP and PTB, can be complicated by bronchiectasis.
Clinical presentation: Chronic cough productive of copious purulent sputum, digital clubbing, focal abnormalities on auscultation, usually coarse crackles, and halitosis.
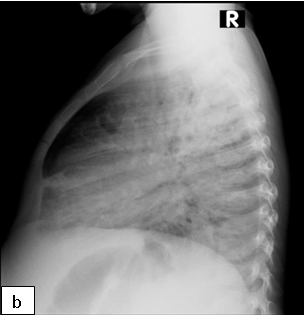
Diagnosis: CXR usually shows focal abnormalities with bronchial dilatation as shown in the figure below. TB may have a similar radiological picture to bronchiectasis and in a high TB burden area where there is over-reliance on radiological diagnosis for PTB, bronchiectasis may be missed or frequent retreatments of TB may occur. Almost a quarter of a cohort of children with HIV-related bronchiectasis in one study received two courses of antituberculosis treatment. In a high TB burden area, the differential diagnosis of an abnormal chest X-ray in children with chronic cough or previously treated TB should include bronchiectasis.
Where available a High-resolution computed tomography (HRCT) scanning is the standard test for diagnosis especially in the absence of characteristic chest radiograph findings of dilated airway, with thickened airway walls. Key features on CT scan: Enlarged internal bronchial diameter with bronchi that appear larger than the accompanying artery. Other findings include the failure of the larger airways to taper while progressing to the lung periphery, air fluid levels in the dilated airways, and the identification of airways in the extreme lung periphery. Other testing may be indicated to diagnose underlying conditions.
Treatment: Broad spectrum antibiotics to treat recurrent infections and chest physiotherapy. Long-term low dose therapy with azithromycin has been found to be beneficial in patients with bronchiectasis as it has anti-inflammatory effects but was accompanied by increased carriage of azithromycin-resistant bacteria in one study.