Kaposi sarcoma and Non-Hodgkin lymphoma are two of the greatest contributors to malignancy burden among HIV-infected children. KS is an AIDS defining disease that typically occurs with lower CD4 count and high viral load.
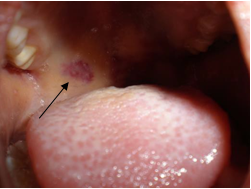
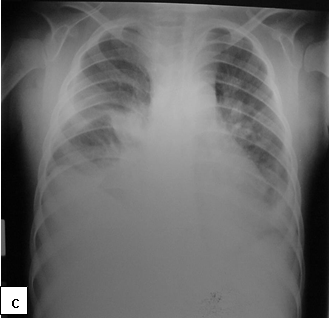
Clinical presentation:Cutaneous lesions are the most common manifestations of KS, presenting as non-tender, purplish and indurated lesions. KS may also involve the lymph nodes, oral mucosa and the lungs. Visceral dissemination can occur, occasionally without skin lesions.
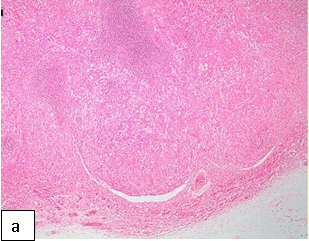
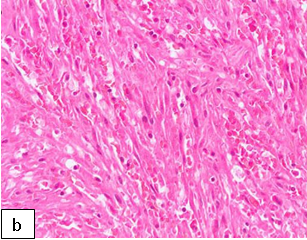
Diagnosis:Diagnosis is confirmed on histology which shows chronic granulomatous changes with cellular neoplasm composed of spindle cells with slit-like spaces containing red blood cells.
Histoimmunochemistry test may be positive for HHV 8 which further confirms the diagnosis of KS.
Differentials:Pyogenic granuloma, tuberculosis, lymphoma, bacillary angiomatosis and dermatofibromata
Treatment:ART is the first line of management. ART may lead to regression of the lesions but referral for chemotherapy (vincristine and bleomycin or liposomal preparations of danorubicin and doxorubicin) in an experienced cancer-treatment centre is usually required for extensive lesions.
Further reading:
Cox CM, El-Mallawany NK, Kabue M et al. Clinical characteristics and outcomes of HIV-infected children diagnosed with Kaposi Sarcoma in Malawi and Botswana. Pediatr Blood Cancer 2013; 60 (8):1274-80. doi: 10.1002/pbc.24516
Saka B, Mouhari-Toure A, Wateba IM et al. AIDS related Kaposi sarcoma: 103 cases in dermatology in Lomé (Togo). Med Sante Trop. 2013; 23(1):109- 11. doi: 10.1684/mst.2013.0145.
Oladokun RE, Kolude B, Ogun GO et al. Kaposi sarcoma in HIV positive Nigerian Children: A case series. World J AIDS 2011; 1(3), 63-69.
Chagaluka G, Stanley C, Banda K et al. Kaposi's sarcoma in children: an open randomised trial of vincristine, oral etoposide and a combination of vincristine and bleomycin. Eur J Cancer. 2014; 50(8):1472-81. doi: 10.1016/j.ejca.2014.02.019.
Figure 161: (a) almost complete replacement of the nodal tissue by (b) a proliferation of spindle cells with slit-like vascular spaces. (Courtesy: Dr. Komala Pillay. Paediatric pathologist, Red Cross Children’s Hospital, Cape Town).Figure 162: Kaposi sarcoma lesion (black arrow).Figure 163: Kaposi sarcoma on the sole of the right foot.Figure 164a and b: Fungating eye tumour and lymph node in an 8 year old child with late diagnosis of HIV. Histology confirmed the lesion to be Kaposi sarcoma.Figure 165a, b and c: Kaposi sarcoma involving the skin, lymph nodes and lungs (Courtesy of Dr George Chagaluka, Queen Elizabeth Central Hospital, Malawi).
Non-Hodgkin's Lymphoma (NHL)
HIV-infected patients are at increased risk of developing non-Hodgkin lymphoma compared with the general population. Highly active antiretroviral therapy reduces the incidence of AIDS-related non-Hodgkin lymphoma and improves overall survival. NHL cases with HIV are highest for diffuse large B- cell and Burkitt lymphomas.
Further reading:
Sungari P, Santilli V, Cotugno N et al. Raising awareness of non-Hodgkin lymphoma in HIV-infected adolescents: report of 2 cases in the HAART era. J Pediatr Hematol Oncol. 2013 Apr;35 (3):e134-7. doi: 10.1097/MPH.0b013e318282cef5.
Shiels MS, Engels EA, Linet MS, Clarke CA, Li J, Hall HI, Hartge P, Morton LM. The Epidemic of Non-Hodgkin Lymphoma in the United States: Disentangling the Effect of HIV, 1992-2009. Cancer Epidemiol Biomarkers Prev. 2013; 22(6):1069-78.
Carreira H, Lorenzoni C, Carrilho C et al. Spectrum of pediatric cancers in Mozambique: an analysis of hospital and population-based data. Pediatr Hematol Oncol. 2014; 31(6):498-508.
Davidson A, Wainwright RD, Stones DK et al. Malignancies in South African children with HIV. J Pediatr Hematol Oncol. 2014; 36 (2):111-7.