
Antiretroviral therapy has greatly reduced morbidity and mortality from HIV infection. One of the complications of immune recovery following ART is IRIS which occurs especially in the first weeks of initiating therapy and majorly in patients with severe immunosuppression. Compared with adults, information on IRIS in children is limited. Incidence of IRIS in children varies between 6 and 21% depending on geographic location and case definition.
Clinical presentation: The onset of IRIS is usually acute and there are features of inflammation, which may be generalized (e.g., fever, tachycardia) or localized (e.g., lymphadenitis).
Paradoxical IRIS - Symptoms and signs associated with an opportunistic infection (OI), for which treatment is underway, recur or become acutely worse, despite an earlier improvement to therapy prior to ART.
Unmasking IRS - A new previously undiagnosed OI presents, unmasked by the immune recovery following ART initiation.
Conditions associated with IRIS in HIV infection:
Diagnosis: Diagnosing IRIS is a challenge as there is no definitive diagnostic test for it. There should be evidence of a favourable response to ART, indicated by a falling HIV viral load. With limited laboratory support in developing country settings, IRIS is usually a diagnosis of exclusion after clinicians have treated multiple conditions that may be thought to be responsible for worsening the patient’s condition.
In the absence of contraindications, use of corticosteroids, for more severe forms of mycobacterial and fungal-associated IRIS (but not for viral-associated IRIS) may be beneficial.
IRIS may be prevented by optimal prophylaxis of OI in advanced HIV (e.g., co-trimoxazole to prevent PCP) and optimal screening and appropriate treatment for subclinical or clinical OI (e.g., TB screen prior to ART initiation)
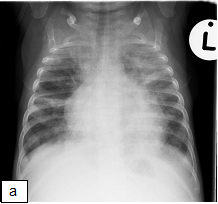
X-ray shows: Progressive air space disease with new more confluent left lower lobe, right lower lobe and right upper lobe consolidation plus a large pleural effusion with dense opacification of the left upper lobe as before.
