Distal radius fractures
by Ntambue Kauta & Stephen Roche
Learning objectives
- Understand radiologic measurements to describe a distal radius fracture.
- Know the indications for surgical intervention.
- Know the conservative treatment.
Introduction
Distal radius fractures follow a bimodal distribution. The low energy distal radius fracture affects older, often female, patients living with osteoporosis. The high energy distal radius fracture affects young individuals.
The clinical assessment follows the same principles of advanced musculoskeletal injury assessment.
Low energy distal radius fracture
Often an extra-articular fracture, displaying a consistent displacement pattern, including dorsal angulation, shortening, radial deviation, and radial tilt. This is the so-called Colle’s fracture, and patients typically present with a ‘dinner fork’ deformity of the wrist. When the angulation is volar, it is called Smith’s fracture.
The treatment is initially conservative. A closed reduction to reverse the deformity must be conducted, and a well moulded below-elbow plaster applied
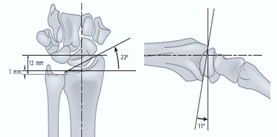
The radiographic criteria for an acceptable reduction of a distal radius fracture are:
- Radial length of more than 5mm.
- Radial inclination angle of more than 15o.
- Sagittal articular tilt of less than 7o dorsal tilt.
Patients are reviewed fortnightly for a fracture position check. The cast should be removed after six weeks and followed by physiotherapy.
High energy distal radius fracture
These fractures are often intra-articular and comminuted. They may present with soft tissue compromises such as open wounds or blisters.
After an initial assessment, a closed reduction should be attempted to alleviate soft tissue pressure from displaced fragments. Fractures that fail conservative treatment as per the criteria above and open fractures must be referred for surgery.