Lower limb soft tissue injuries
by Kirsty Berry, Shaun De Villiers & Marc Nortje
Learning Objectives
- Have an approach to lower limb soft tissue injuries.
- Diagnose common soft tissue injuries in lower limbs.
- Understand the basic management principles of these injuries.
Introduction
Ligament, tendon and muscle injuries of the hip, knee and ankle are common conditions seen in emergency departments and general practice. The majority of these injuries can be treated with conservative management. It is essential to identify injuries that should be referred to an orthopaedic surgeon for possible surgical intervention or further work-up.
Groin injuries
Also known as an adductor strain.
Clincial Findings
History
Most often young athletes complain of groin pain following an injury while playing sport (most often running). It is more common in males than in females.
Examination
- Tenderness in the groin.
- Antalgic gait.
- Pain on resisted adduction of the hip, passive end of range abduction of the hip (adductors stretched), or both.
Additional injuries to note
It is essential to rule out non-orthopaedic causes such as inguinal hernias.
Special investigations
Imaging
- X-rays are normal.
- MRI – show changes in the adductor (oedema or tear); most often not indicated.
Management
Non-Surgical
- RIC(E):
- Rest
- ICE
- Compression
- Physiotherapy for rehabilitation and return to activity.
Surgical
Rarely indicated.
Ligament and meniscal injuries of the knee Applied anatomy

The stability of the knee is dependent on bony anatomy, joint capsule, ligaments, menisci and surrounding muscle. The most commonly injured structures in the knee are the ligaments and menisci that can lead to ongoing pain, difficulty with daily and sporting activities and instability. The ligaments of the knee are the anterior and posterior cruciate ligaments and medial and lateral collateral ligaments. Both medial and lateral menisci contribute to stability function and articulation of the knee joint. Image 1 shows the anatomy of the ligaments and menisci.
Clincial Findings
History
- Anterior cruciate ligament – the typical history is twisting the knee with the ankle fixed and immediate swelling.
- Posterior cruciate ligament – an anterior force to the tibia in a flexed knee. Dash-board injury is the most common mechanism.
- Medial (MCL) and lateral (LCL) ligament injuries – valgus (MCL) or varus (LCL) force applied to the knee
- Multi-ligament injuries – most often seen in high-velocity motor vehicle accidents or patients with a high BMI and low-velocity injuries.
- Meniscal injuries – the typical history is twisting motion on the fixed ankle with delayed swelling.
Examination
- Look
- Swelling is typical of all injuries around the knee.
- Feel
- Joint effusion may be seen with all injuries and can be assessed with the patella tap test. Tenderness over the MCL or LCL collateral may indicate an injury in this area. Anterior lateral or medial pain on palpation may point to lateral or medial meniscal injuries, respectively.
- Move
- Range of motion of the knee may be limited (normal 0–130).
- Anterior and posterior draw test – ACL and PCL
- Lachmann and reverse Lachmann – ACL and PCL
- Varus and valgus stress tests – lateral and medial collateral ligaments, respectively
- McMurray’s meniscal injuries
Additional injuries to note
- May be associated with vascular injuries (especially in multi-ligament injuries); vascular assessment is essential.
- High suspicion of reduced knee dislocation in patients with multi-ligament knee dislocations.
- Poly-trauma patients must be assessed closely in the case of a swollen knee and normal X-rays
Special investigations
Imaging
- Plain film X-rays may be normal.
- Horizontal beam lateral (HBL) view may show an effusion (lipohaemarthrosis).
- Stress views are useful in diagnosing ligament injuries (compare to the contralateral side).
- Soft tissue swelling can be seen on plain film X-rays.
- An MRI is the gold standard for assessing soft tissue injuries.

(A)

(B)
Management
Non-surgical
- Rest
- Ice
- Compression
- Elevation
- Crutches with partial weight-bearing for pain management
- Analgesia (including NSAIDs where indicated)
Surgical
- Failure of conservative management in the non-athlete, with ongoing pain and instability after six weeks.
- Multi-ligament knee injuries.
- ACL and meniscal injuries.
- Surgery includes arthroscopic or open repair or reconstruction of ligaments; debridement, repair or replacement of menisci.
Achilles’ tendon rupture
Applied anatomy
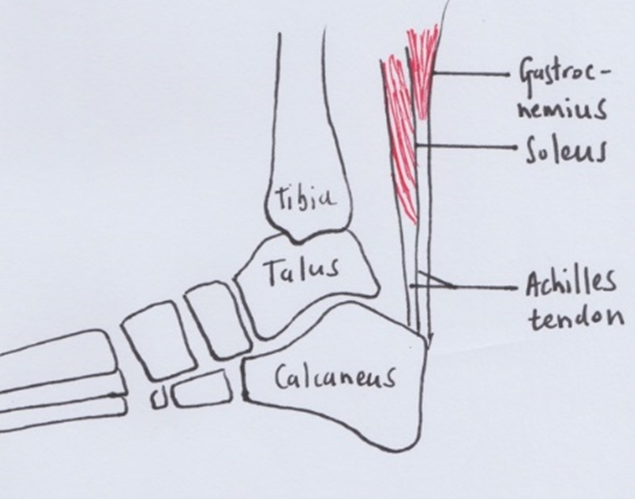
The Achilles tendon is the confluence of the soleus and gastrocnemius muscles of the posterior compartment of the leg. It inserts onto the posterior aspect of the calcaneus tuberosity. Its primary function is plantar flexion of the ankle joint.
Clinical findings
History
Most often, a low-velocity injury. The foot is either forced into extreme plantarflexion or dorsiflexion from a maximal plantarflexed position. A popping sound may be heard at the time of injury. The patient may have pain in the heel or calf and difficulty walking. The so-called ‘weekend warrior’ is vulnerable to this type of injury. The use of fluoroquinolones and steroid injections around the ankle has been associated with Achilles’ tendon rupture.
Examination
- Tenderness and ecchymosis around or proximal to the insertion of the tendon.
- A gap in the tendon on palpation.
- Inability to actively plantarflex.
- Thompson test – pathognomonic.

Differential diagnosis
- Ankle sprain
- Ankle fractures
- Calcaneus fractures
Special investigations
Imaging
- X-rays are normal.
- Ultra-sound – confirm the clinical diagnosis; determine the size of the gap and differentiate between partial and complete tears.
- MRI – helpful if the clinical diagnosis is unclear or for surgical planning in chronic tears.

Management
All patients with Achilles’ tendon rupture should be referred to an orthopaedic surgeon.
Non-surgical
Serial casting progressing from plantar flexion to neutral every two weeks for 6–12 weeks has shown good outcomes in the low demand patient with acute tendon rupture.
Surgical
- An open or percutaneous repair can be considered for closed injuries.
- Open injuries with direct laceration rather than tear should be repaired primarily.
- Tendon reconstruction and transfers are surgical options in chronic tears.

Ankle sprain
Applied anatomy
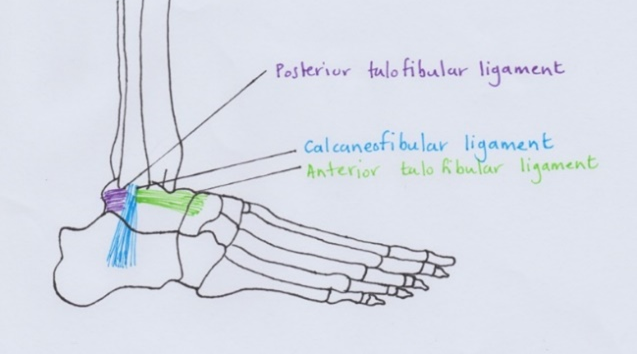
Ankle sprains involve injury to the lateral ligament structures of the ankle, specifically the anterior talofibular (ATFL) and the calcaneofibular ligaments (CFL).
Clinical findings
History
Inversion on a plantarflexed foot. The patient often reports ‘twist of the ankle’.
Examination
- Oedema and ecchymosis around the lateral aspect of the ankle
- Tenderness over the lateral ankle (both lateral malleolus and talus).
- Inability to weight-bear.
- Anterior draw test for the ankle may be positive.
- Talar tilt test – inversion (especially end of range) causes pain.

Additional injuries to note
- Fractures of the ankle (lateral malleolus) and tarsal bones (especially talus and calcaneus) must be ruled out.
- Syndesmosis injuries can present as high ankle sprains (positive squeeze test).
Special investigations
Imaging
- X-rays – normal bony anatomy; soft tissue swelling may be evident.
- MRI – only indicated in chronic injuries or where the diagnosis is unclear.
Management
Non-surgical
- The majority of injuries improve with non-surgical intervention. The mainstay of treatment is ‘RICE’:
- Rest
- Ice
- Compression
- Elevation
- Non-weight or partial weight-bearing for pain relief.
- Physiotherapy
Surgical
- Indicated where conservative measures have failed.
- Arthroscopy of the ankle for diagnosis and debridement of the joint.
- Repair or reconstruction of the ATFL or tendon rerouting.
Essential takeaways
- Ankle strains are the most common of all lower limb soft tissue injuries.
- History and clinical examination are essential for diagnosis.
- Non-surgical management of these injuries is the mainstay.
- Achilles’ tendon ruptures and ligament and meniscal injuries to the knee should be referred to an orthopaedic surgeon for further assessment and possible surgical intervention.
References
Martin et al, 2014. AAOS Comprehensive Orthopaedic Review, Volumes 1 and 2. USA. American Academy of Orthopaedic Surgeons
Assessment
- A 24-year-old male rugby player is injured during a game when his foot is locked on the ground, and his knee is twisted. The knee swells up immediately, and he is unable to bear weight. The most likely structure injured is:
- Posterior cruciate ligament
- Medial meniscus
- Anterior cruciate ligament
- Lateral collateral ligament
- Patella tendon
- A 54-year-old male is running at his daughter’s school in the father-daughter race. Halfway down the track, he hears a pop and is unable to continue running. Which of these is not a risk factor for Achilles’ tendon rupture:
- Systemic steroid use
- Course of ciprofloxacin for UTI a week ago
- Cortisone injection into the tendon two weeks before the injury
- Age
- Alcohol consumption
- A 20-year-old gymnast twisted her ankle following landing off the bar apparatus. She has swelling, ecchymosis and pain on the maximal passive inversion of the foot. What is the next most appropriate management for her injury:
- Immediate referral to an orthopaedic surgeon.
- Weight-bearing – continue to excercise through the pain and re-assess in a week.
- Early anterior talofibular ligament repair.
- Ice pack over the area, compression bandage with Robert Jones-type bandage, crutches for non-weight bearing and no gymnastics.
- Tendon rerouting surgery to prevent recurrence and early return to sport.
(C) is correct, as this is the typical history described by the patient with an acute ACL injury
(E) is correct – alcohol has not been linked to Achilles’ tendon rupture. All the others are known risk factors. A Cortisone injection should never be given due to the risk of rupture.
(D) is correct, as the majority of all ankle sprains can be treated conservatively