Femur Fracture
by Michael Abrahamson & Graham McCollum
Learning objectives
- Emergency management of femur fractures.
- Signs of fat embolus syndrome.
- Correctly communicate the injury to the team.
Introduction
Femur fractures are usually a result of high energy injuries. A high index of suspicion for other injuries is essential.Close adherence to advanced trauma life support (ATLS) principles is critical. An adult can lose up to two litres of blood following a femur shaft fracture and early,aggressive resuscitation is paramount.
Check closely for open wounds. Any laceration on the affected leg should be treated as an open fracture and managed accordingly. A femur fracture is a clinical diagnosis, and the initial splinting and resuscitation should be initiated before obtaining X-rays. You don’t need an X-ray.
Clinical findings
History
Mechanism and time of injury, past medical history (smoker, diabetics or other comorbidities, job requirements).
Examination
ATLS. Examine for other injuries and perform a neurovascular examination. A careful examination of the pelvis (including pelvis and PR stability if there is pelvic tenderness) is mandatory). C-spine should be protected in high energy injury until cleared clinically. Assess for hypovolemic shock.
Exclude Fat Embolism Syndrome (FES) (Chapter: Orthopaedic emergencies)
Additional injuries to note
Depending on the mechanism of injury, it is vital to exclude spine, pelvis, tibia and chest injuries, especially for high energy injuries. Focus on potentially lethal injuries first (open pelvis, tension pneumothorax, cardiac tamponade,multiple long bone fractures, unstable c-spine)
Imaging
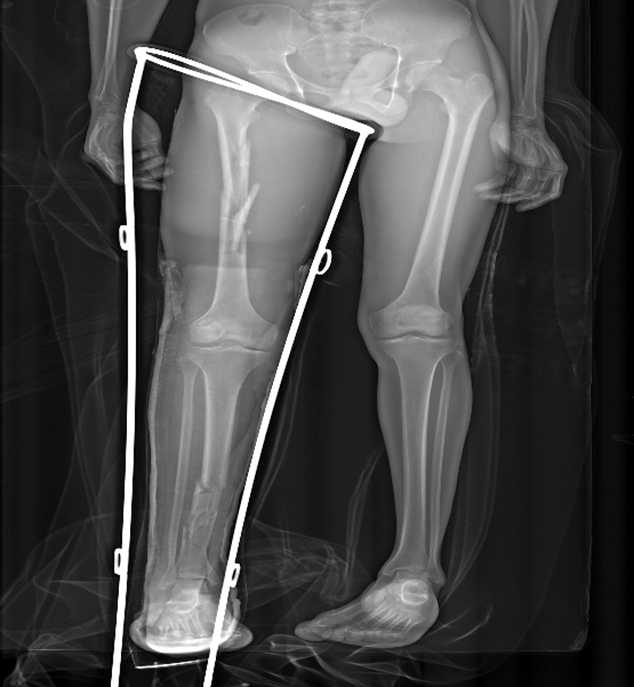
Two views are needed (AP and lateral,joint above and below included). A Thomas splint should be applied BEFORE X-ray. Exclude neck of femur fractures which occur in 10% of femur shaft fractures.
Classification
It is essential to communicate the fracture with the team and to document the injury adequately. Documentation should be done based on:
- The anatomic area of the fracture:diaphysis, metaphysis, intra- articular.
- Fracture pattern: simple, complex (comminuted), spiral, oblique, transverse.
- Communicate, ‘LARA’ parameters for conservative treatment do not apply to the femur (length, apposition, rotation, angulation).
Management
- Early resuscitation, including fluids and analgesia. Aim for a mean arterial pressure >60mmHg.
- A Thomas splint must be applied to all femur shaft fractures before X-rays (reduced blood loss, pain and FES).
- There is a very limited role for conservative treatment (unless the patient is not fit for theatre).
- For initial stabilisation, skin traction in the form of a Thomas splint is indicated for comfort and to decrease the need for blood replacement therapy. Skeletal traction and ‘balanced traction’ is an option if delays of more than 12h are anticipated before the patient can receive surgical management.
- Most femur fractures will need osteosynthesis, either with an intramedullary (nail) or extramedullary (plate) fixation.

Essential take-aways
- Femur fractures are high energy injuries.
- A Thomas splint and fluid resuscitation save lives.
- The majority of patients need surgery.
Assessment
What is the most critical urgent strategy in femur fractures?
- Call an orthopaedic surgeon.
- Apply a Thomas splint.
- Manage fluids.
- Administer morphine.
(B) is correct, as a Thomas splint reduces blood loss, pain and risk for FES.