Fractures of the forearm and wrist
by Anria Horn
Learning objectives
- Identify and describe forearm fractures in children.
- Manage Monteggia and Galleazi fractures.
- Understand conservative management of forearm fractures.
- Gauge acceptable deformity in paediatric forearm fractures.
Forearm fractures in children
- Very common fracture.
- Caused by a fall on an outstretched hand (FOOSH) with a rotational component. Single bone fractures are usually a result of direct trauma.
- Present with clinical deformity, pain and swelling.
- Exclude neurological and vascular compromise.
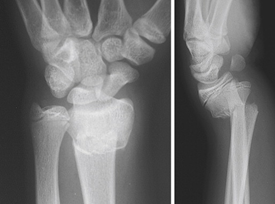
- X-rays: AP and lateral including wrist and elbow.
- Must exclude Monteggia and Galeazzi fractures.
Fracture description:
- Complete vs incomplete (greenstick) vs plastic deformity.
- Open vs closed.
- Distal vs diaphyseal vs proximal
- Shortening
- Angulation (apex volar/dorsal/radial/ulnar)
- Translation
- Rotation
Monteggia and Galeazzi fractures
The radius and ulna form a ‘ring’ of sorts. Therefore, shortening and marked angulation of the one bone has to be accompanied by fracture of the other bone OR dislocation on either end of the unbroken bone.
Useful mnemonic: GRUM - Galeazzi Radius Ulna Monteggia
Monteggia fractures
This is a displaced ulna fracture, usually proximal, with a radial head dislocation. To identify a radial head dislocation, check that the capitellum and radial head are aligned on AP and lateral X-rays.


Galeazzi fractures
Isolated radial fracture with distal ulna dislocation.
Extremely rare in children as distal ulna physeal fracture more likely.
The treatment for Galeazzi and Monteggia fractures usually involves anatomical reduction and fixation of the fractured bone. This leads to spontaneous reduction of the dislocated joint. These fractures should always be referred urgently.
Conservative management of paediatric forearm fractures
The majority of paediatric forearm fractures can be managed conservatively in plaster, with or without closed reduction.
All fractures proximal to the distal radial physis should be immobilised in an above-elbow cast to control elbow movement.
Due to remodeling, certain degrees of angulation, shortening and rotation can be accepted.
Acceptable degrees of deformity in paediatric forearm fractures
| ≤ 9 years | ≥ 9 years | |
|---|---|---|
| Distal forearm | 25° | 15-20° |
| Mid and proximal shaft | 15° | 10° |
| Rotation | 0° | 0° |
| Shortening | 1cm | 1cm |
Reduction of displaced / angulated fractures
- Check the neurovascular status of the limb and document it.
- The patient needs to be sedated and relaxed.
- The deforming force needs to be reversed. Most commonly this requires traction and flexion (volar angulation).
- Three-point moulding is employed to ensure maintenance of the reduction once achieved.
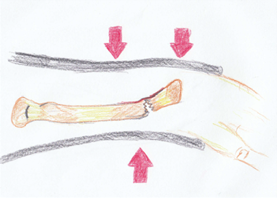
Three-point moulding for apex volar fracture - Interosseus moulding will help restore the radial bow.
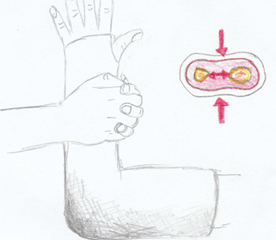
Interosseous moulding - X-rays are performed to confirm adequacy of reduction
- Patient is observed for a few hours to exclude features of compartment syndrome.
- NB: Educate parents regarding elevation, swelling and warning signs of compartment syndrome.
- Arrange follow-up after one week to check the position of the fracture.
What to do if excessive swelling/ features of compartment syndrome:
- Elevate the limb.
- Encourage finger movement.
- Split/bivalve the cast and the padding.
- Refer urgently if no alleviation of symptoms.
Indications for referral and surgery
- Unacceptable deformity following attempted closed reduction.
- Recurrence of deformity.
- Open fractures.
- Pathological fractures.
- Neurological or vascular compromise.
- Galeazzi and Monteggia fractures.
- Older children (≥ 13) with limited remodeling potential.