Lower limb injuries in children
by Stewart Dix-Peek & Benjamin Blankson
Learning objectives
- Identify and diagnose lower limb paediatric fractures.
- Institute emergency management protocols for the fracture in an acute setting.
- Understand the definitive management protocols for various lower limb fractures.
Introduction
Fractures make up about 10–25% of all injuries in the paediatric population1. Of these, lower limb fractures make up approximately 15.9%2 and the prevalence increases with age1,2. These are mostly due to high-energy trauma from motor vehicle accidents (MVAs), sports injuries, falls from heights and non-accidental injuries (NAI) among others2. A study conducted in the Red Cross War Memorial Hospital revealed falls from height (39%) as the major cause of femur fractures in the toddler group (peaking at 2 to 3 years). Next was MVA peaking at 4 to 5 years (33.7%); struck by foreign objects (11%); NAI, pathological fractures and sporting injuries followed in descending order3. This chapter will focus on highlighting lower limb fractures in a child and various protocols for management. Generally, patients need to be assessed initially and stabilised according to ATLS principles.
Specific injuries
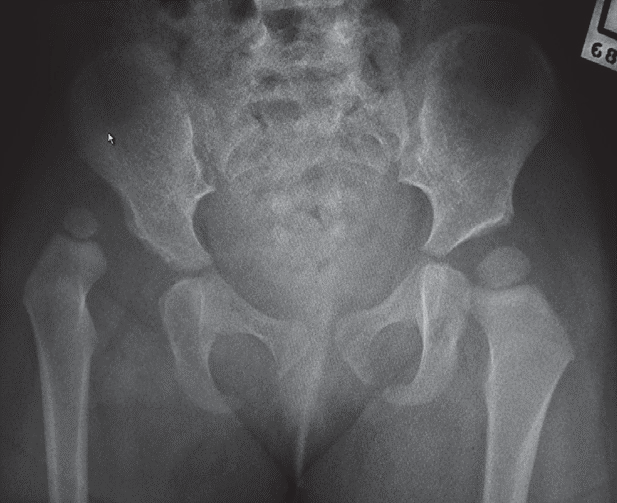
Hip fracture
Overview
Hip fractures are rare in children. They usually occur from high-energy trauma, particularly MVA and a high index of suspicion is needed to diagnose them. X-ray (AP and lateral views) are essential to make the diagnosis, and a CT scan may be indicated for occult fractures. Below is a table summarising how hip fractures are classified.
| Classification | |
|---|---|
| Type I | Transepiphyseal fracture, with or without dislocation of the femoral head. |
| Type II | Transcervical. Usually displaced. |
| Type III | Cervicotrochanteric |
| Type IV | Intertrochanteric |
Treatment
- Acutely immobilise in traction
- Type I:
- Closed reduction with smooth pin fixation in the younger child or cannulated screws or threaded pins in the older child.
- If closed reduction is not possible,
- open reduction is indicated.
- Type II and III
- Undisplaced: spica cast.
- Displaced: closed reduction and cannulated screws. In the younger child, avoid crossing the physis with screws, and if closed reduction fails, open reduction is indicated.
- Type IV:Traction in abduction, or open reduction and internal fixation if irreducible or unstable.
Hip dislocation
Overview
Posterior dislocations account for 80% of hip traumas. Low energy injuries cause traumatic hip dislocations in the younger child (2–5 years) due to associated ligamentous laxity. In older children (11–15years), dislocated hips are caused by higher energy injuries and have a higher association with acetabular fractures, although this is rare. Dislocations are more common than fractures in the paediatric population.
Clinically
- Posterior dislocation:Typically flexed, adducted, internally rotated hip.
- Anterior dislocation:Typically extended, abducted, externally rotated hip.
Conduct a careful neurovascular evaluation with particular attention to the sciatic nerve. Ipsilateral femoral shaft fracture should be excluded before manipulation.
Investigations
If an acetabular fracture is identified on the pre- or post-reduction X-rays, Judet (45° obturator and iliac oblique) views should be obtained. If an intra-articular fragment or incongruent reduction is present, a CT scan is indicated.
Treatment
Exclude an ipsilateral femur fracture before reduction. Assess neurovascular status (especially sciatic nerve function) both before and after reduction. Acutely, attempt closed reduction under procedural sedation, as this is usually successful. In delayed or neglected cases, traction for 3–6 days should be attempted before open reduction if an initial attempt of closed reduction was unsuccessful. Once the hip is reduced, immobilise in traction for 4–6 weeks.
Open reduction is rarely necessary; surgical intervention is indicated in:
- Failed closed reduction
- Nonconcentric reduction
- Displaced acetabular fractures
- Intra-articular fragments
- Sciatic nerve palsy occurring post- reduction where it was normal before reduction.
Complications
- Avascular necrosis (3–15%) decreased incidence under age 5
- Nerve injury - sciatic or gluteal nerve
- Coxa Magna - not associated with functional limitation
- Redislocation
Femoral shaft fractures
Overview
Femoral shaft fractures present with a bimodal distribution peaking at 2–4 years and mid-adolescence, predominantly in males. In the neonate, fractures are mainly due to birth trauma and non-accidental injury. In children under one year, 50% are due to non-accidental injury and, in adolescents, most are due to MVA.
Classification
| Descriptive | Anatomical |
|---|---|
|
|
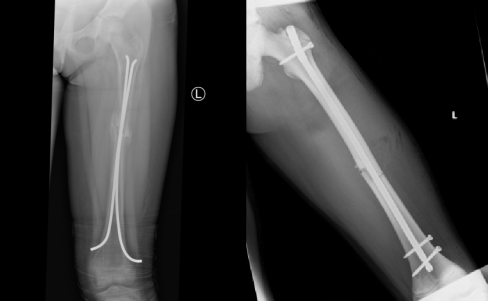
Treatment
The table below summarises the accepted angulation in a femur fracture.
| Age | Varus/valgus | Anterior/posterior |
|---|---|---|
| 0–2 years | 30° | 30° |
| 2–5 years | 15° | 20° |
| 6–10 years | 10° | 15° |
| >11 years | 5° | 10° |
Below are guidelines to management of femur shaft fractures; however, these may vary between facilities, depending on the preference and expertise of the surgeons.
| Age | Treatment | Duration | Comments |
|---|---|---|---|
| Neonates | Pavlik harness | 3 weeks | |
| <2yr / <12kg | Gallows traction | 3–6 weeks | Compartment syndrome risk |
| 2–8 years | Early spica cast | 4-8 weeks | |
| 8–12 years | Traction | 6–8 weeks | |
| Retrograde IM nails | Partially weight bearing to full as pain permits | Removal at 6 months | |
| >12 years | Prograde IM nails | Trochanteric entry point. Locked nail | |
| Special circumstances | |||
| Compound fractures | External fixator/plate with preliminary debridement, antibiotics | ||
| Severe head injury | ORIF (done once patient’s condition stabilised) | ||

Complications
- Malunion:Remodelling will not correct any rotational deformity. Younger patients remodel better than older patients, and sagittal plane deformities remodel better than coronal plane deformities.
- Non-unionis rare. Should it occur, bone graft and plate or IM nail fixation is indicated.
- Limb length discrepancy:As a result of either shortening or overgrowth. 1 cm of overgrowth can usually be expected, and early shortening of 1–2 cm is acceptable. Up to 2 cm of leg length discrepancy is well tolerated.
- Avascular necrosis of the femoral head:may occur with antegrade nailing of femoral fractures through the piriformis fossa. For this reason, a trochanteric approach is recommended before skeletal maturity.
Knee injuries
Overview
In the immature skeleton, physes fail before ligaments under tensile load. Ligamentous injuries are therefore uncommon before skeletal maturity. Two-thirds of the longitudinal growth of the lower limb occurs in the distal femur (10 mm/year), followed by the proximal tibia (6 mm/year). Injuries to the physes may lead to premature growth arrest or angular deformity.
Distal femur fracture
Ligamentous and tendinous structures insert on the epiphysis, leaving the physis unprotected. Injury is usually due to indirect forces: varus/valgus hyperextension/hyperflexion, usually resulting in a Salter-Harris II type injury.
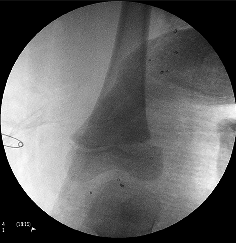
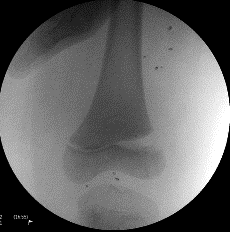
Radiological evaluation
AP and lateral films should be ordered. Oblique views are needed when in doubt or to visualise the fracture better. Stress views may be necessary to identify undisplaced fractures. In infants, separation of the distal femoral physis may be missed. The ossified centre of the epiphysis should always be in the line of the femoral anatomic axis on AP and lateral.
Classification
| Salter-Harris | Displacement |
|---|---|
| Type I:Easily missed. Stress views may be necessary. | Hyperextension injury – anterior |
| Type II:Most common type. Usually varus or valgus injury. | Hyperflexion injury – posterior |
| Type III:Intra-articular. Often best seen on AP X-rays as the physeal component is in the sagittal plane. | Varus injury – medial Valgus injury – lateral |
| Type IV:Rare injury but a high incidence of linear physeal bar formation. | |
| Type V:Diagnosis usually made retrospectively. |

Treatment
- Undisplaced fractures:Above-knee POP with the knee in extension
- Hyperflexion injuries:MUA and maintain position with above-knee POP with the knee in extension
- Hyperextension injuries:MUA impractical to maintain reduction by keeping knee flexion; therefore, cross-pin using smooth k-wires or Steinmann pins from the epicondyles to the metaphysis.
- Varus/valgus injuries:MUA and cross pins
- With Salter-Harris III and IV injuries, open reduction is necessary to restore the articular congruity unless the fracture is undisplaced.
In the older child with a large metaphyseal spike (Thurston-Holland fragment), the fragment may be used to maintain reduction with cannulated lag screws.
Complications
Early
- Vascular injury:Usually with hyperextension injury. The cool, pulseless foot pre-reduction requires urgent reduction. If it resolves, it requires observation for 48–72 hours to exclude intimal tears. The cool pulseless foot post-reduction requires urgent angiography.
- Peroneal injury:This is usually associated with varus injuries. The patient should be put in an ankle-foot orthosis until the nerve recovers to prevent an equinus foot deformity. Persistent nerve palsy at three months should be evaluated with electromyography and possibly exploration.
Late
Physeal closure: 50% of physeal injuries in the distal femur will result in arrest. This is due to the interdigitating nature of the distal femoral physis. The physeal injury will present with a bar manifesting as angular deformity or limb length discrepancy.
References
Modified images:
Dislocated hip. Available from:
https://commons.wikimedia.org/wiki/File:Dislocated_hip.jpg
{kind=link}