Tuberculosis of the spine
by Robert Dunn
Learning objectives
- Identify clinical features of spinal tuberculosis.
- Recognise imaging features of spinal tuberculosis.
- Approach to definitive diagnosis.
- Understanding medical therapy and surgical indications.
Introduction
Tuberculosis (TB) is a devastating infection in the developing world with 10.4 million new cases and 1.8 million deaths globally in 2015. South Africa has one of the highest prevalences at 1%, predominately in the socio-economic poorer communities, but TB is increasingly seen among immigrants in the Western world. In Sub-Saharan Africa the co- existence of HIV drives the disease further. TB reaches the musculoskeletal system by haematogenous spread in roughly 5% of cases, half of which result in spinal tuberculosis (sTB).
Clinical presentation
Patients with a history of immune- comprise from malnutrition and particularly HIV are at increased risk. Known contacts increase the likelihood, but with the widespread prevalence patients may not be aware of their contact.
Constitutional symptoms of weight loss, fatigue and night sweatsmay be present. There is an insidious onset of back pain in the area of involvement, most commonly thoracic. The pain is often not severe until late and spinal destruction has occurred. There may be radicular pain radiating around the chest or down the legs depending on thoracic or lumbar involvement, respectively. When there is advanced abscess formation or bony collapse and spinal cord compression, patients will experience progressive weakness and deteriorating ambulatory function, with associated loss of sensation and eventually incontinence.
On examination they may be cachectic but surprisingly many remain overweight despite the chronic illness. They may be pyrexial but often not. There may be a draining sinus over or adjacent to the spine, groin or a fluctuant mass. There may be evidence of a gibbus, i.e. posterior bony prominence of the exaggerated spinous process due to vertebral body destruction, collapse and kyphosis.

A neurological examination may reveal a sensory level, below which there is altered or absent sensation indicating the level of disease. Motor involvement will confirm this. Depending on the level of spinal cord involvement and stage of disease, the neurological status may initially be flaccid before becoming more typical upper motor neuron like with spasticity.
Diagnostic workup
Basic bloods may reveal an anaemia of chronic disorders – normocytic, normochromic. The white cell count is invariably normal in contrast to pyogenic infections. There may be a lymphocytosis on the differential until associated with HIV, when there may be a lymphopaenia. The platelets are often raised. In children a provocative intra-dermal inoculation with attenuated TB (Mantoux, Tine, Heaf) may indicate active disease if there is an excessive response at 48 hours. Unfortunately due to BCG vaccination and likely exposure in the community, all patients will respond making interpretation qualitative. Likewise very ill patients with suppressed cellular immunity may not respond despite having active disease.
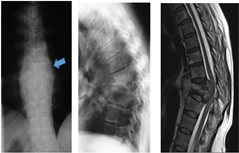
A chest X-ray may confirm associated active pulmonary TB; it is generally not the case, but subtle evidence of previous TB may be evident. AP and lateral spine X-rays may be normal in early disease but unlikely as most present late. The typical features are para-spinal abscess, para-discal vertebral body collapse and kyphosis. This differentiates sTB from pyogenic discitis where the latter is usually far more painful, earlier disc destruction with disc height loss and minimal bony destruction. A CT scan may be useful in delineating bony destruction, but generally a MRI is far more useful as it confirms the paraspinal abscess, the spinal cord compression and spinal cord signal – which correlate with neurological function. The MRI will also identify non-contiguous lesion seen in up to 16% of sTB.
Differential diagnosis
TB is the great mimicker and can be confused with many other pathologies. It needs to be differentiated from other causes of infection and tumours. Tumours generally involve one body, whereas sTB two (one either side of the disc). However on occasion sTB can involve one body leading to confusion. A large associated abscess on the MRI generally points to TB. Pyogenic spondylodiscitis, staphylococcal aureus and the gram negatives typically cause acute, severe pain, as opposed to the insidious onset of sTB. Bacteria generally cause disc pathology with loss of disc height on X-ray and hyperintense signal in the disc on MRI. The disc is generally preserved until late in sTB. Due to the more acute nature of pyogenic infection, there is less bony destruction and seldom kyphosis. Less commonly parasitic infections such as Hydatid (echinococcus), fungi and rare bacteria such as ‘cat scratch disease’ can cause spine infection. Thus despite TB being common, a wide differential should be obtained.
Definitive diagnosis
A biopsy is mandatory to confirm the diagnosis. This may be done as an outpatient via CT guided biopsy with a suitably large core needle under local anaesthetic and sedation. The yield is operator and sample size dependant. Otherwise an open biopsy can be performed in theatre as an isolated procedure or part of a surgical debridement, spinal cord decompression and reconstruction procedure. Tissue and pus should be sent for MC&S, TB culture, PCR (GeneXpert) and histology. The MC&S will confirm a bacteria cause, whereas TB culture remains the most sensitive and gold standard for TB diagnosis. It unfortunately takes up to 6 weeks for the result, whereas Gene Xpert is 90–95% sensitive and specific in 1–2 days.
Histology is diagnostic if AFBs are seen, which is seldom, as sTB is a pauci-bacterial disease, but suggestive if there are necrotising granuloma present. TB drug sensitivities are confirmed on GeneXpert and culture.
Management
Medical
The mainstay of management is medical with combination agent Rifafour – rifampicin, isoniazid, pyrazinamide and ethambutol. We recommend all drugs for a minimum of 9 months due to the poor penetration of paraspinal pus and granuloma. Should the patient feel clinically better, gain weight, ESR normalise and X-ray show signs of healing (sclerosis), we would stop and observe 3 monthly. Should there be ongoing concern, the drugs would be continued. During this period, vigilance should be maintained for the drug side effects of visual impairment and hepatitis. As vision cannot be assessed in young children, the ethambutol is omitted. In patients with co-existent HIV, the ESR usually remains high and can be ignored if the patient is otherwise improving. During this period dietary optimisation is mandatory.
Surgery
| Surgical indications for sTB |
|---|
|
Surgery with above indications will usually involve resection of diseased tissue, restoration of normal spinal alignment, reconstruction typically with an allograft humeral shaft from the bone bank, and support of the correction with titanium screws and rods. Surgery is always supported by medical therapy. With this approach, almost all spinal TB patients will recover neurologically, even those that have lost full motor and sensory function.