Approach to bone sarcomas
by Thomas Hilton, Len Marais, Nando Ferreira & Luan Nieuwoudt
Learning objectives
- Evaluate a bone sarcoma.
- Formulate a description of a X-ray.
- Develop a radiological differential diagnosis for a bone tumour.
- Outline a basic initial management plan.
- Understand the indications for surgical management and urgent referral.
Case presentation
A 12-year-old female patient presents with a swelling on the left upper arm. The mass was first noted about 2 weeks ago and is painful at rest. She has had no previous trauma to the shoulder region and has no other medical problems. The mother states that she has had a couple of episodes of low-grade fever over the past 2 weeks, without any other symptoms. Examination reveals a large, firm, non-tender mass located deep to the fascia. There is no neurovascular deficit.

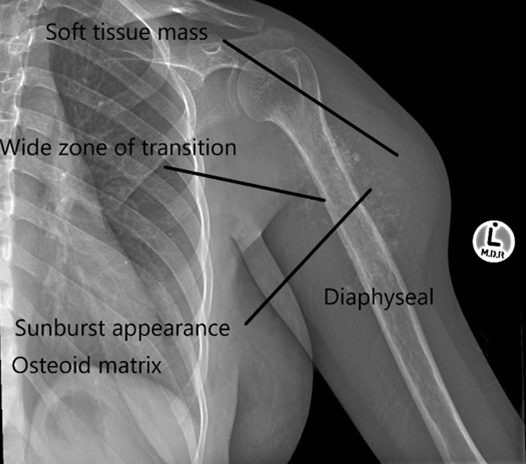
Anterior-Posterior (AP) X-ray of the patient’s left upper arm and shoulder showing a diffuse lytic lesion in its shaft/ diaphysis extending in a centrifugal (in all directions) manner.
Working from the outside in, there is extensive soft tissue extension from the bone, the matrix of the lesion shows cloud-like / ill-defined amorphous ossification in parts. There is a wide zone of transition between the normal bone and diseased bone, meaning that the border between them is not easily defined. The lesion is lytic in nature giving the humerus a moth-eaten appearance.
These are all features of a malignant bone sarcoma.

History
Ask for important components in the history such as:
Duration: How long has the mass been there?
Progression: Is it enlarging? Does it ever decrease in size? Is the size constant?
Associations: Is the mass painful, and if so, when? Any other symptoms associated with the mass? Any fever, night sweats or loss of weight?
Etiology: History of trauma? Symptoms suggestive of infection, i.e. fever, etc?
Previous/other masses? Previous medical history? Previous surgical history?
Examination
Structure your examination into inspection, palpation and movement.
Look
- Site: Determine location of the mass
- Superficial or deep to the fascia?
- Size: width x length x depth
- Shape: What is the shape of the lesion?
- State of overlying skin: Are there any skin changes?
Feel
- Temperature: Does the overlying skin feel warm?
- Consistency: Soft, spongy, rubbery hard, bony hard? Does it fluctuate? Is it pulsatile?
- Margin: Indistinct or clearly defined border?
- Tenderness: Is it tender?
Move
- Surrounding structures: Is it attached to the skin or underlying bone? An intramuscular mass becomes more difficult to feel and less mobile when the muscle in which it is located contracts.
- Any lymphadenopathy?
- Range of motion of adjacent joints.
Regional neurovascular examination
Examine distal pulses and peripheral nerve function.
Systemic examination
- General examination.
- Identify any other areas of involvement (metastases).
Special investigations
Plain film X-rays
On X-rays you will gain important information (see chapter on approach to orthopaedic X-ray). Specifically look for:
- Identify view, patient and date
- Is the patient skeletally mature?
- Single or multiple lesions
- Bone involved
- Part of bone involved (epiphyseal, metaphyseal or diaphyseal?)
- Medullary, cortical or periosteal
- Lytic, mixed or sclerotic appearance
- Appearance of tumour matrix (ossified or calcified)
- Zone of transition (narrow or wide, i.e. clearly demarcated or not)
- Cortical destruction, thinning or expansion?
- Periosteal reaction present?
- Pathological fracture?
- Soft tissue extension?
MRI scan
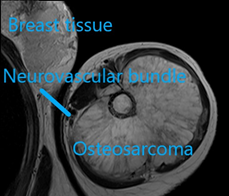
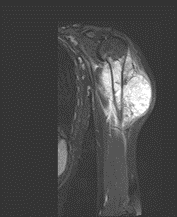
The MRI scan is important to differentiate sarcomas from infections and to evaluate soft tissue components, and the integrity of the neurovascular bundle. This is often a diagnostic modality which is performed at specialised centres.
Systemic staging
A CT scan of the chest and abdomen, as well as a technetium bone scan allow assessment of the patient for skip lesions or metastases and stage the progression of the disease.
Differential diagnoses
Infections (bacterial, TB, fungal, parasitic) and traumatic causes (fracture callus, myositis ossificants, seroma/hematoma) are important differential diagnoses for undiagnosed masses. Benign aggressive tumors of the bone can also be associated with a mass (i.e. giant cell tumour, aneurysmal bone cyst). The most common malignant bone tumors are osteosarcoma, Ewing’s sarcoma, and chondrosarcoma.
Management
- The workup and referral is urgent, as bone sarcomas double in size every 28 days and urgent referral to bone sarcoma unit for further workup and biopsy is mandatory.
- The MRI scan must be done before the biopsy so as not to interfere with the interpretation of the MRI scan.
- Discussion of all investigations in a multi- disciplinary team, including medical oncologists, radiologists, pathologists and surgeons is important to ensure the best outcome for the patient.
- General treatment pathway will include diagnosis and local and systemic staging (looking for metastatic disease), followed by neoadjuvant chemotherapy, followed by surgery and adjuvant chemotherapy.
- Surgical treatment will consist of either tumour resection and reconstruction (limb salvage) or amputation.
- More than 90% of cases are amenable to limb salvage which involves the resection of the tumour with a cuff of normal tissue to minimise the risk of local recurrence and reconstruction of the limb.
- There are many ways to do this but one of the more popular methods is with an endoprosthesis which is inserted into the space left by the tumour to give structure to the limb and allow function. An example is given below.
Essential takeaways
- Young patient with a short history of a large swelling of the body – consider bone sarcoma.
- Deep, firm, non-tender, large mass – consider bone sarcoma.
- Pervasive, wide zone of transition, lytic bone lesion – consider bone sarcoma.
- Urgent referral to bone sarcoma unit for diagnosis and management.
References
- Browse NL. An Introduction to Symptoms and Signs of Surgical Disease. 2nd ed. London, UK: Edward Arnold; 1991.
- Triana F, Errani C, Toscano A, Pungetti C, Fabbri D, Mazotti A, et al. Current Concepts in the Biopsy of Musculoskeletal Tumors. J Bone Joint Surg Am. 2015;97:e7(1-6).
- Puri A. The principles of surgical resection and reconstruction of bone tumours. Orthop Trauma. 2010;24(4):266- 75.