Common bone tumours
by Thomas Hilton, Len Marais, Nando Ferriera & Luan Nieuwoudt
Learning Objectives
- Identify common benign and malignant tumours.
- Understand treatment pathway for benign and malignant bone sarcomas.
- Appreciate urgency and importance of early, appropriate referral.
Introduction
As a general rule, bony lesions are rare. They are broadly divided into benign (non-cancerous) and malignant (cancerous) growths of connective tissue. Malignant lesions are termed sarcomas. This is different to the malignant growths of epithelial cells, termed carcinoma. They behave very differently from each other. Sarcoma is present in many different ways, shapes and forms. The underlying principle is to refer the patient to a specialist centre for management. Never assume the growth is nothing to worry about. Anything bigger than a golf ball must be considered malignant until proven otherwise. Urgent referral is important as the doubling time of a sarcoma is 28 days and the work-up to make the diagnosis and stage the patient can be lengthy, further delaying treatment. The sooner treatment is started, the better the outcome.
Applied anatomy
Sarcomas arise from a particular connective tissue cell and their histopathology is often given a diagnosis according to the cell line they develop into. For example, an osteosarcoma is a malignant tumour of a bone forming cell as it resembles bone, although not quite the same, under the microscope. Sarcomas grow centrifugally in a uniform and outwards direction and respect fascial barriers (these divide muscles and vital structures into compartments). They are also heterogenous in nature, which means that an osteosarcoma will have many different areas behaving in a different manner which is not uniform throughout. Also, an osteosarcoma in one patient is very different to an osteosarcoma in another patient in terms of is growth, location, metastatic potential, etc. This makes them very hard to study and is very different to carcinomas, which are uniform in nature and have invasive growth that does not respect fascial barriers.
Definition of terms
Lesion – A region in an organ or tissue which has suffered damage through injury or disease.
Benign – Not harmful.
Malignant – Cancerous
Chemotherapy – Classically intravenous cytotoxic treatment designed to kill cancer cells.
Neoadjuvant chemotherapy – Chemotherapy given before surgery.
Adjuvant chemotherapy – Chemotherapy given after surgery.
Biopsy – Sampling of a tumour to obtain a histopathological diagnosis.
Lytic/lysis – The disintegration of tissue by a process. In bone this means a cavity is formed and on X-ray this looks darker when compared to surrounding bone.
Sclerotic/sclerosis – abnormal hardening of tissue. On X-ray this looks more white/ dense when compared to surrounding bone.
Classification
One of the more common systems used is the Enneking classification system.
Benign tumours are split into
Latent – e.g. enchondroma or non-ossifying fibroma
Active – e.g. unicameral bone cyst or osteoblastoma
Aggressive – e.g. aneurysmal bone cyst or giant cell tumour of bone
Malignant tumours are graded according to histological percentage of cellular atypia. Intra vs extra compartmental involvement as well as metastases present (or not) are also taken into account.
Assessment
History
- Bone tumours are often slow growing, non-tender and located deep, which leads to late detection.
- Pain can point towards a risk of fracture or compression of neurological structures
- Function may be compromised if the mass located juxta-articular.
- Constitutional symptoms are not always present, but include night sweats, fever, loss of weight, cough.
Examination
- A general examination should evaluate wasting, anaemia (lymphadenopathy usually not present as sarcomas do not spread through lymphatic system primarily).
- A local examination should assess for skin changes. The mass is usually deep, firm, immobile and non-tender. Large masses > 5cm should be taken seriously.
X-rays
Certain tumors have specific features on X-rays. Below are the most common tumours and their appearances.
Benign bone tumours
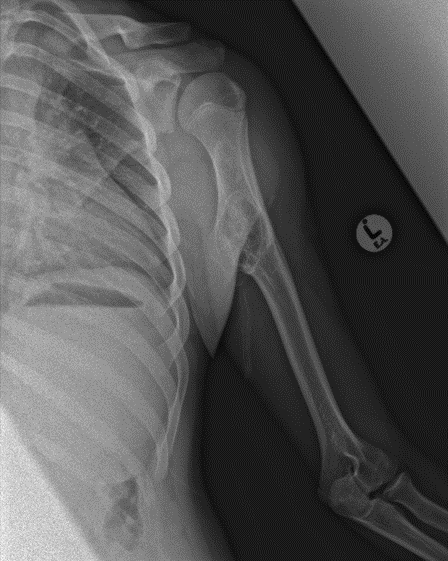
Osteochondroma.A common and benign cartilage lesion affecting young people. Often on the surface of bones or near tendons around the knee, proximal humerus or proximal femur.
Aneurysmal bone cyst (ABC). A benign neoplastic lesion with multiple blood- filled cavities and a membranous inner lining. Must be differentiated from a sub-type of osteosarcoma called a telangiectatic osteosarcoma. This is a malignant lesion of bone and the treatment is very different for each lesion.
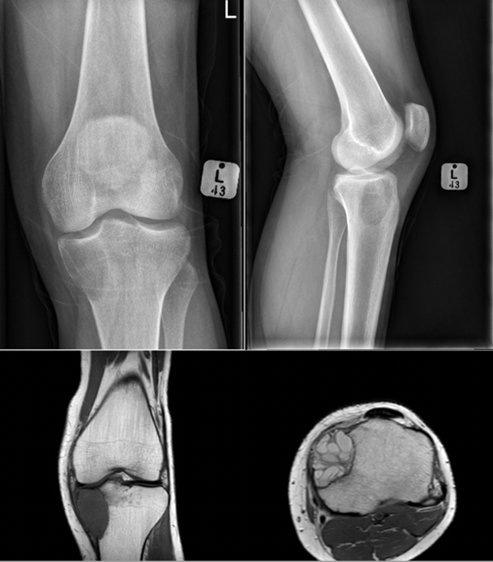
Giant cell tumour: A benign aggressive lesion of bone that has a soap bubble appearance on X-ray. Often found around the knee. It is usually metaphyseal and eccentric in the bone. It is named after its predominant cell type, which is of course the giant cell.
Malignant bone tumours

Osteosarcoma. There are many types of osteosarcoma but the most common is the classic intramedullary type which usually originates from the intramedullary cavity of the metaphyseal area of long bones. It is the most common type of bone sarcoma overall. It is most often found in teenagers and young adults. Any pathological fracture in a young person must be considered malignant until proven otherwise. The treatment of an osteosarcoma is classically neoadjuvant chemotherapy – surgery – adjuvant chemotherapy. The biopsy to diagnose bone sarcomas should be done by a sarcoma specialist to prevent difficulties with future surgery and spread of the tumour locally. The 5-year survival for patients with osteosarcoma is between 60% and 70%.

Ewings sarcoma. The most common bone sarcoma found in children. This lesion is often diaphyseal and described as having an onion skin like appearance on X-ray. It is also found commonly on flat bones such as the scapular, ribs and bones of the pelvis. It is very sensitive to chemotherapy and also radiotherapy which is unusual for a bone sarcoma.

Chondrosarcoma.A primary malignancy of bone composed of chondrocytes or cartilage cells which have a varying degree of malignancy. The appearance on X-ray is often described as popcorn-like due to the calcification of areas in the tumour. This tumour can be treated in many ways depending on a biopsy, so it is best to refer the patient to a specialist centre. The MRI scan is important to differentiate sarcomas from infections and to evaluate soft tissue components, and the integrity of the neurovascular bundle. This is often a diagnostic modality which is performed at specialised centres.
Management
Non-surgical
Enneking latent (e.g. enchondroma) require no active management. Surveillance is occasionally advised.
Enneking active (e.g. unicameral bone cyst) can include observation or local treatment, which usually includes a marginal curettage (scraping away of the lesion) and adjuvant therapy, i.e. bone cement/graft, phenol
Enneking aggressive (e.g. ABC or GCT) usually require treatment which can range from marginal curettage to endoprosthetic replacement.
Surgical management

Curretage and bone grafting. The above images show an aneurysmal bone cyst of the left calcaneus. This is represented by a lytic process that looks soap bubbly on the initial X-rays. Because the patient is young and it is a benign lesion, a curettage and bone grafting has been performed. The series of X-rays following the bone grafting show the body’s incorporation of the graft, replacing it with the patient’s own bone.

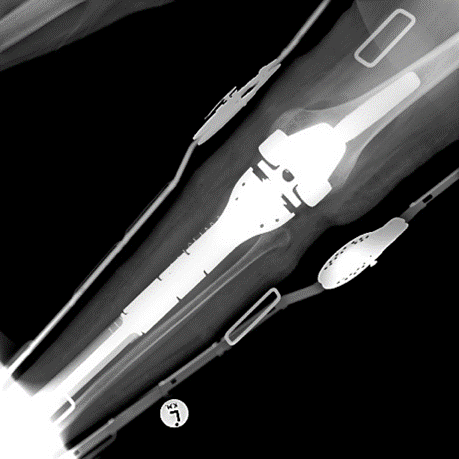
Endoprosthetic replacement. An example of a wide local resection of a patient who had an osteosarcoma of her proximal tibia. The initial X-rays show the pervasive lytic lesion of the proximal tibial diaphysis and metaphysis. The subsequent X-rays show an endoprosthetic replacement called a proximal tibial replacement. The knee has been replaced with a hinge-type knee replacement and the bone and tumour of the proximal tibia has been replaced by a modular metal prosthesis with a stem cemented into the distal femur and the proximal tibia.
Essential takeaways
- Sarcomas arise from connective tissue, are rapidly growing and heterogenous in nature.
- They are divided into benign and malignant conditions.
- Early referral to a specialist unit is imperative.
- Benign lesions are usually observed or treated locally.
- Malignant lesions will require staging, work-up for surgery and chemotherapy and wide resection of the tumour with adjunctive oncological treatment.
References
- Browse NL. An Introduction to Symptoms and Signs of Surgical Disease. 2nd ed. London, UK: Edward Arnold; 1991.
- Triana F, Errani C, Toscano A, Pungetti C, Fabbri D, Mazotti A, et al. Current Concepts in the Biopsy of Musculoskeletal Tumors. J Bone Joint Surg Am. 2015;97:e7(1-6).
- Puri A. The principles of surgical resection and reconstruction of bone tumours. Orthop Trauma. 2010;24(4):266- 75.