Acute tendon injuries
by Pieter Jordaan, Neil Kruger & Ian Koller
Learning Objectives
- A penetrating wound associated with a deficit in tendon function should be regarded as an acute injury to either the tendon or nerve supplying the muscle-tendon unit.
- Thorough knowledge of anatomy and hand function is essential to recognise these injuries.
- All suspected tendon injuries should be referred for specialist review.
Definition and anatomy
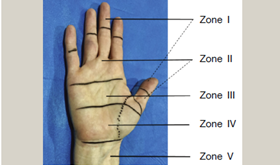
Any injury leading to tendon dysfunction should be assessed for a tendon injury. The specific forearm anatomy and function of each tendon will not be discussed here, but it should be revised to understand tendon injuries better. Tendon injuries are broadly divided into extensor and flexor injuries subdivided into zones. Injuries in the proximal forearm that result in tendon dysfunction are more likely to be nerve injuries.

Mechanism of injury
In the majority of cases, the mechanism of injury is penetrating trauma. Closed tendon ruptures occur in Mallet finger injuries, acute Boutonniere deformity, EPL rupture in distal radius fractures and extensor tendon ruptures in rheumatoid arthritis.
Differential diagnosis
- Nerve injury leading to dysfunction (nerve and tendon injury often coexist).
- Pain inhibition.
- Underlying fractures or dislocations.
Diagnosis
The diagnosis is made by taking a good history and examining each tendon individually
History
Patients with penetrating hand or forearm injury will usually present due to the recent trauma. In closed ruptures, patients may give a history of preceding pain, followed by acute worsening pain or feeling of tearing, associated with a sudden loss in function.
Examination
Look for the specific area of the laceration which will guide you as to what injuries to expect.
For the extensor tendons, there will be an evident extensor lag (inability to extend the digit fully) or resisted extension will be weak or painful. This can also indicate a partial injury. The tendon injury may be some way from the entrance wound in penetrating trauma. It may even be on the other side, for example, flexor injuries from a dorsal stab that penetrates the interosseous membrane
The Mallet injury (closed extensor rupture of the insertion on the distal phalanx) causes an inability to extend the distal phalanx actively. An acute Boutonniere deformity (closed rupture of the central slip off the base of the middle phalanx) is a rare injury. It is associated with a weak extension of the middle phalanx confirmed with Elson’s test.
For the flexor tendons, each tendon should be examined individually, including FDS and FDP of each finger. Closed flexor ruptures are rare, but can be associated with inflammatory conditions (RA) or following plating of distal radius fractures or can occur as a Jersey finger (a closed injury where the FDP insertion avulses of the base of the distal phalanx). Flexor tendon injuries are often associated with nerve injuries, and these should be actively excluded.
Certain injuries will leave no functional deficit, for example, an injury to palmaris longus or if only a single wrist extensor or flexor has been injured.
Special investigations
You do not need special investigations to diagnose acute tendon injuries. A baseline X-ray should be performed to exclude underlying fractures or retained foreign bodies. If there is doubt about a closed rupture, an ultrasound may be useful.
Management
All suspected tendon injuries should be referred.
Non-surgical
- Closed Mallet and Boutonniere injuries can be managed in a splint.
Surgical
- All other tendon injuries are managed with surgical repair or reconstruction and a strict therapy regime. Outcome after surgery depends significantly on the patient’s compliance with rehabilitation instructions.
- If no rehabilitation is available, the patient should be referred to a specialist centre as repair without post-operative rehabilitation is of minimal benefit to the patient.
Complications
- Stiffness and permanent functional impairment.
Pitfalls
- Missing tendon injuries due to a lack of careful examination of each individual tendon or insufficient knowledge of anatomy.
- Missing associated nerve injuries or underlying fractures.
References
Hammert WC, Calfee RP, Bozentka DJ, Boyer MI, 2010. ASSH Manual of Hand Surgery; Lippincott, Williams and Wilkins (Wolters Kluwer); Philadelphia, USA.
Jordaan PW, Watts AC. Acute tendon injuries; Orthopaedics and Trauma 2019; 33(1): 54–61
Miller MD, 2008. Review of Orthopaedics, 5th edition; Elsevier; Philadelphia, USA.
Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, Cohen MS, 2017. Green’s Operative Hand Surgery, 7th Edition; Elsevier; Philadelphia, USA.
Assessment
A 20-year-old male presents with a stab wound to the back of his hand and inability to extend his index finger. What tendon or tendons has he injured?
- EPL
- EDC to the index finger
- EIP
- EDC to the index finger and EIP
- EDC to the index finger, EIP and ECU
The correct answer is (D), EDC to the index finger and EIP.