Orthopaedic emergencies
by Stephanie Roche, Kim Laubscher, Stefan van der Walt & Stephen Roche
Learning Objectives
- Red flags in the outpatient setting: infection, malignancy and spinal disorders.
- Red flags in the Orthopaedics ward: fat embolism, compartment syndrome, Paediatrics: non-accidental injury.
Orthopaedic red flags
Many orthopaedic problems can be managed in the primary care setting. To practice safely at this level of care, medical officers need to know which patients to investigate and follow-up and when to refer patients for urgent or emergency management.
Initial assessment includes a thorough history of the presenting complaint and medical history (particularly concerning trauma, cancer, immunosuppressive conditions or medications), and a musculoskeletal and neurological examination. The crucial warning signs on history and examination that suggest serious pathology and which might warrant referral or specialist advice, are listed in the table.
| Clinical red flags | |
|---|---|
| History: | |
| Local |
Rapidly progressive symptoms Red, hot swollen joint Pain interrupting sleep |
| Systemic |
Loss of appetite Loss of weight Fever Change in bowel or bladder function Weakness or change in sensation History of cancer History of intravenous drug use Immunosuppression |
| Examination |
Fever >38oC Inability to bear weight on joint Red/hot /swollen joint Saddle anaesthesia Lower motor neuron signs Reduced anal tone Bilateral upper motor neuron signs |
Malignancy
Malignant tumours of soft tissue and bone should be excluded in all patients with a mass or lesion with any of the characteristics listed in the table. Imaging (ultrasound for soft tissue masses, radiograph for bony masses) and referral to a specialist should be the next step. See the specific chapter for more information.
| Red flags for masses |
|---|
| Rapid growth |
| Pain |
| > 5cm diameter |
| deep to fascia |
Infection
Primary septic arthritis and osteomyelitis are important differentials in patients presenting with musculoskeletal pain or swelling. Delay in diagnosis (even by hours) can result in progressive joint destruction. Importantly, obvious signs of inflammation may be absent in immunosuppressed patients, and investigations may be warranted in the absence of systemic signs. In immunocompetent patients, one or more of the following features listed in the table alongside are present.
Diagnosis
- Blood results as above (WCC, ESR or CRP, blood culture).
- Uric acid and inflammatory arthritis markers. Gout and inflammatory arthritis will be on the list of differentials and may need to be excluded.
- Synovial fluid aspiration (assess the appearance of fluid, cells and differential count, crystals, Gram stain and culture) –
- X-rays
Differential diagnosis:
- Inflammatory arthritis, for example, rheumatoid arthritis, psoriatic arthritis (although more likely oligo- or polyarthritis, as opposed to monoarthritis)
- Osteoarthritis
- Gout, pseudogout
- Trauma (for example, haemarthrosis)
For treatment, please refer to the respective chapter on infections.
| Red flags for infections | ||
|---|---|---|
| Systemic |
Temperature Leukocytes Respiratory rate Heart rate |
>38°C >12 000 x 109/L elevated elevated |
| Orthopaedic | Inability to weight bear | |
| Blood results |
ESR CRP |
>40mm/ hr elevated |

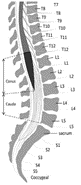
Spinal pathology
In addition to the general red flags mentioned at the beginning of the chapter, the following features may also suggest serious spinal pathology. Patients presenting with signs of cord compression or cauda equina syndrome (see figure below) need urgent referral to an orthopaedic or neurosurgical service.
| Red flags for spinal disorders | ||
|---|---|---|
| History |
- Back pain in a patient < 20 or > 55 years of age. - Previous history of cancer - Immunosuppression - Thoracic pain - Pain at rest or at night - Neurological fallout - Structural deformity |
|
| Cord compression | Upper motor neuron symptoms: - Increased muscle tone - Brisk reflexes - Clonus - Weakness |
|
| Cauda equina | Lower motor neuron symptoms: - Sphincter disturbance, bladder or bowel changes, -gait abnormalities, saddle anaesthesia, sexual dysfunction, decreased tone or weakness of lower limbs, absent reflexes, diminished or absent anal wink test and a bulbocavernosus reflex |
|
Fat embolism syndrome
Definition: Fat embolism is a rare, non- thrombotic embolism that is potentially fatal and has a mortality rate of 15%. It is a systemic dysfunction caused by the entry of fat into the circulation, most commonly from the bone marrow. The mechanism of entry into the systemic circulation is thought to be due to either a patent foramen ovale or via microembolism, where the fat particles are small enough to pass from the pulmonary arteries into the pulmonary veins. Patients typically develop fat embolism as a result of long bone fracture or orthopaedic surgery. It occurs 12 hours to 2 weeks following trauma or surgery. The diagnostic criteria in the following table can be used.
Management: Supportive treatment with frequent ICU admission is required.
| Clinical features of fat embolism Gurd and Wilson criteria: 2 major or 1 major and 4 minor criteria = FES |
|
| Major |
|
|---|---|
| Minor |
|
Compartment syndrome
Compartment syndrome results from increasing pressure in an anatomical compartment (typically muscle compartments divided by strong fascia), where the tissue pressure exceeds the vascular perfusion pressure. The tissue becomes ischaemic and infarction will occur without urgent intervention.
Clinical features:
Can occur after any form of injury, but most commonly associated with long bone fractures or other forms of trauma
The leg's anterior compartment is most frequently affected (e.g. after tibia fracture), but any compartment can be affected (e.g. hand or forearm).
Early symptoms include pain, paraesthesia and swelling. Often the pain is out of proportion to what is expected from the injury. These symptoms occur as venous pressure is exceeded. Late symptoms include the other Ps: paralysis, absent pulses, pallor and poikilothermia (or cold peripheries). These symptoms occur as arterial pressure is exceeded.
The diagnosis is clinical; the management is urgent fasciotomy.

Deep vein thrombosis
Deep vein thrombosis (DVT) occurs when there is thrombus formation in one of the deep veins, typically of the lower limb or pelvis.
Thromboembolism to the pulmonary vasculature (pulmonary embolism) is the most feared complication and is potentially fatal. Importantly, Orthopaedic post-surgical patients are at a greater risk of DVT due to the nature of the operation ( hip and pelvic surgery, for example) and because these patients are often older and immobile.
Clinical features:
- Unilateral leg swelling with or without associated erythema and distended superficial veins
- Pain (often worse on dorsiflexion of the foot)
- Warmth and tenderness on palpation
- Shortness of breath, chest pain, or both in pulmonary embolism cases (always look for a DVT in patients who develop respiratory symptoms in the ward).
Diagnosis: Compression ultrasonography
Management: DVTs can mostly be prevented with early mobilisation, compression stockings and pharmacological prophylaxis. Treatment involves anticoagulation therapy with heparin and warfarin.
Non-accidental injury in a child
The red flags listed at the beginning of this chapter should also be applied to children. Every child with a painful or swollen joint should be assessed as to whether they appear systemically unwell or not, and the degree to which they can weight bear or use the affected limb. Orthopaedic and non-orthopaedic red flags are listed in the table below.
Management
Clear, accurate and thorough documentation of all findings, which may also include sketches. By law, all suspected child abuse must be reported to the relevant authorities ( police, social worker, and so on). See the specific chapter in the section on fractures in children for an approach to these patients.
| Red flags for child abuse |
|---|
| Multiple fractures at different stages of healing. |
| Fractures other than the skull or clavicle in neonates (may occur during birth). |
| Severe skull fractures in children under 18 months. |
| Long bone fractures in infants not yet walking. |
| Digital fractures in children under three years. |
| Sternal, rib or scapula fractures (suggest high energy force). |
| Vertebral body fractures. |
| Metaphyseal corner fractures (occurs when a limb is pulled, twisted or shaken). |
| Epiphyseal separations |
| Inconsistent history, lack of witnesses for the incident or clinical findings inconsistent with the reported mechanism of injury.. |
Open fractures
Irrigate, stabilise and administer appropriate early antibiotics. See the chapter on ‘Orthopaedic Injuries’.

References
Amboss. Nonthrombotic embolism, 2019.Available: https://www.amboss.com/us/ Department of Health. Standard Treatment Guidelines and Essential Medicines List for South Africa. (Cellphone application, most recently updated 2019)
Kearon C, Bauer KA, 2018. Clinical presentation and diagnosis of the nonpregnant adult with suspected deep vein thrombosis of the lower extremity. Available [Online in UpToDate]: https:// www.uptodate.com/contents/clinical- presentation-and-diagnosis-of-the- nonpregnant-adult-with-suspected-deep- vein-thrombosis-of-the-lower-extremity
Luqmani R, Joseph B, Robb J, Porter D. Textbook of orthopaedics, trauma and rheumatology. Elsevier Health Sciences, Dec 20, 2012.
Rasul AT, 2018. Acute compartment syndrome. Available: https://emedicine. medscape.com/article/307668- overview#a3
Scherl SA, 2019. Orthopedic aspects of child abuse. Available [Online in UpToDate]: https://www.uptodate.com/contents/ orthopedic-aspects-of-child-abuse
Stracciolini A, Hammerberg EM, 2018. Acute compartment syndrome of the extremities. Available [Online in UpToDate]: https://www.uptodate.com/ contents/acute-compartment-syndrome-of- the-extremities
Weinhouse G, 2019. Fat embolism syndrome. Available [Online in UpToDate]: https://www.uptodate.com/ contents/fat-embolism-syndrome