


Qhamani Maqungu, Sudesh Sivarasu
ORCID ID: 0000-0002-8327-3797, 0000-0002-0812-568x
Division of Biomedical Engineering,
Department of Human Biology,
University of Cape Town,
Western Cape,
South Africa
Anaphylaxis has propelled the use of adrenaline autoinjectors (AAI) globally. This is to ensure patients administer themselves whenever they experience an allergic reaction, anywhere, to reduce the severe consequences that would result if medical services far located far. Common issues identified with AAI: They are forgotten, not simple to use, and often misplaced. This paper proposes a connected mobile system with an e-cap for AAI using wireless communication protocol, Bluetooth. The hardware in this paper comprises of an Arduino nano BLE module, LED, and magnetic buzzer. Several algorithms for tracking were used and quadratic line of best-fit, produced better distance approximation. The accuracy of the system was affected by electromagnetic interferences. Further development is required to improve the robustness of the system using other wireless technologies and algorithms.
Keywords: fast-locating, Bluetooth tracking, smart autoinjector, Bluetooth Low Energy (BLE)
Anaphylaxis is a severe allergic reaction that is triggered by some food products (like peanuts), insect stings or rubber latex (Posner & CA, 2017). In a world with food of diverse cultures, shared recreational areas, the exposure to allergens is almost unavoidable. The disease affects critical physiological systems that are essential for human survival. These systems include cardiovascular, digestive, and the respiratory system. When the reaction occurs, common symptoms including hives, skin rashes, hypotension, nausea, and difficulty breathing, are present before it becomes deadly to the patient.
Anaphylactic patients intramuscular inject epinephrine via autoinjectors (AI) to mitigate the reaction as shown in Figure 1. AAI are injection devices designed to be portable for out-of-hospital use by patients. The adrenaline (epinephrine) is administered in the thigh for fast absorption. Patients are still required to visit an emergency room (ER) even after successful administration of the drug, to avoid biphasic reaction (Levin, et al., 2015).
Given that most available AAI, are mechanical spring-loaded, patients encounter issues when using these devices, including injecting themselves in the thumb instead of thighs (Potera, 2015). Furthermore, patients may not always carry the device with them (Sheikh, Simons, Barbour & Worth, 2012). In the panic before or after using the device, patients may fail to request medical follow-up, putting them at risk (Sheikh, Simons, Barbour & Worth, 2012).
It was found that a delayed administration of epinephrine is less effective as patients will suffer from asphyxia (Pumphrey, 2004). The delay is commonly due to patients not having the AAI within reach. Consequently, eight patients died despite having epinephrine administered within 30 minutes (Pumphrey, 2004).
Short-range tracking technology is used in most household portable items. Smart tags have utilised Bluetooth Low Energy (BLE) and Ultra- wideband (UWB) technology for tracking purposes. An APPhylaxis app enables a patient to locate their AAI smart case using a smartphone. The current AI market players have no device available that calculates distance between a patient and AAI itself, and ultimately inform emergency personnel when the AAI is triggered. The literature, however, discuss accessory devices including smart cases, and sleeves for AAI that provide either one or both features.
BLE is classified as Bluetooth 4.0 and above. The application of these devices is IoT- (Internet of things) related since they consume little energy. In this application, the hardware (BLE) is enclosed in a cap, that forms part of the AAI tip. The Global Positioning System (GPS) is used for locating an object on earth using satellites. GPS modules can come as stand-alone or are found in smartphone devices. Geolocators are power-consuming and need rechargeable, high-density power sources. In this paper, the smartphone is used as host for the GPS system to exploit the rechargeability feature.
The mobile application provides a communication interface between a patient, the hardware, and healthcare providers. The application provides the patient's location in Google Maps. It shows nearby pharmacies with available AAI for patients experiencing an allergic shock.
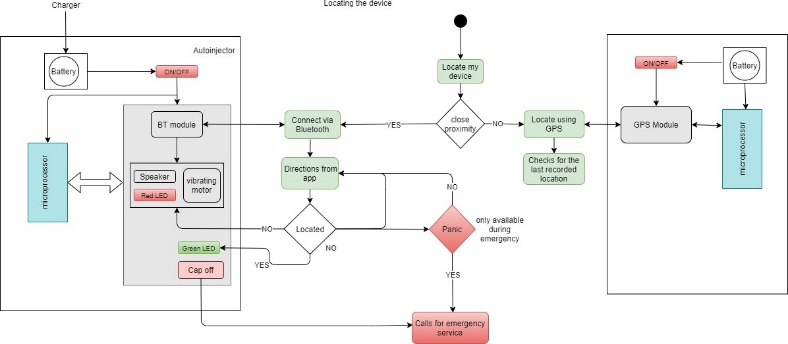
In the design and development, the system consisted of two sub-systems: the hardware, and the mobile application. A readily available development board was used, and the enclosure was 3D-printed. The overall system functional flow diagram is shown in Figure 2.
An Arduino nano BLE 33 was chosen as the microcontroller as shown in Figure 3. This device does not only provide access to nRF52840 microcontroller but has an on- board BLE module, NINA B306 which is based on the nRF52840 Cortex processor. A magnetic buzzer, connected via an NPN transistor, and an RG LED, and a power switch were added peripherals to the development board. A humansafe buzzer that can be heard up to a distance of 10 meters, with an 80dB noise level was used as suggested by (Birgitta, et al., 1999), which is in compliant with ISO 1900.
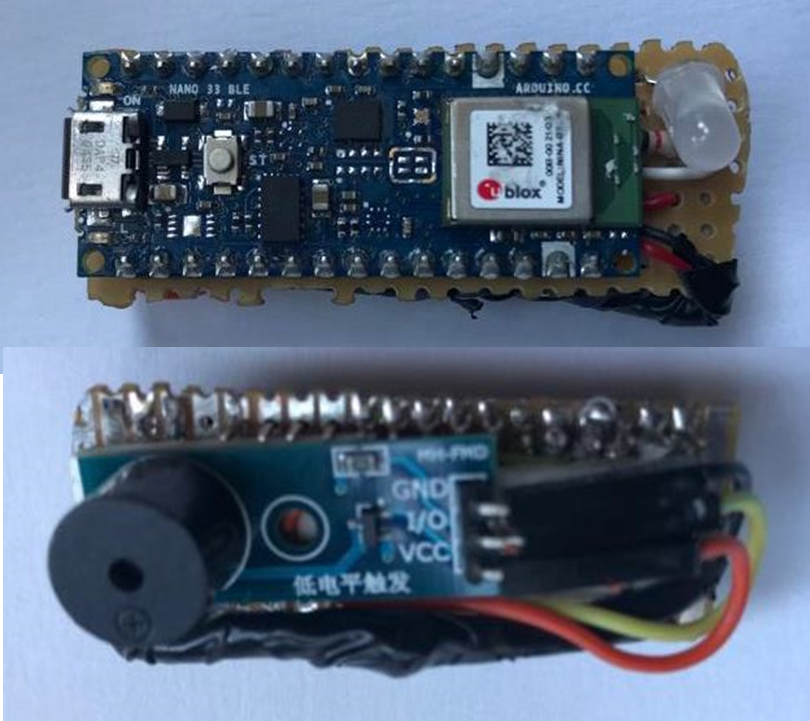
A power bank was used as the power source, with the specifications: Li-polymer, 5000mAh, with output parameters, 5V/200mA. The RG LED was used for successful (green), and termination (red) of Bluetooth connection.
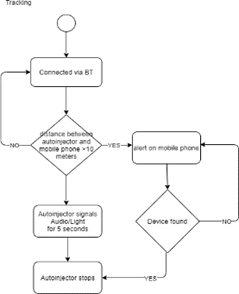
The mobile application was developed in Kotlin, for Android devices. For database storage, Google Firebase was utilised for security and reliability. A flow diagram of the app for Bluetooth tracking is shown in Figure 4.
To get distance, the received signal strength indicator (RSSI) was converted using methods to be discussed. The RSSI value is given in dBmW, which is how much milli watt power in a radio signal is transferred over a meter distance. The RSSI value at one meter was recorded multiple times and averaged to a value of -51 dBm. This value was used to normalise the RSSI values at different points to minimise deviation results.
The best line of fit was generated on the data using a natural logarithm and a quadrating equation, as shown with Equation 1 and Equation 2 respectively.
𝑑𝑖𝑠𝑡𝑎𝑛𝑐𝑒 = 𝑒(𝑅𝑆𝑆𝐼𝑟𝑎𝑡𝑖𝑜−𝐾) (1)
𝑑𝑖𝑠𝑡𝑎𝑛𝑐𝑒 = 𝑎𝑥2 + 𝑏𝑥 + 𝑘 (2)
Local notifications are triggered when the patient is located far from the AAI. The patient is provided options to fast locate the device on the app using a panic button feature or follow the distance approximated by the app, in case of an emergency. The options include ringing a buzzer and controlling an LED or reading numbers off the mobile app showing how far the device is from the patient, respectively.
Logarithm estimation proved to be less accurate compared to the quadratic polynomial estimation. Therefore, the quadratic method was implemented (Equation 2). It created less fluctuations when a patient was constantly moving. Shown in Figure 5 below.
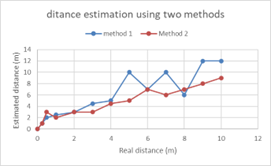
An accurate estimation should produce a straight-line positive correlation. From the graphs, method two (quadratic equation) was chosen to be the final iteration for this method. These results were influenced by electromagnetic interference, i.e., Wi- Fi, Bluetooth, or microwaves. Bluetooth had more influence on the signal. Other factors included:
The method, however, was implemented on the mobile application for testing. The geo-location was implemented successfully using google maps and it produced accurate geo-pinning, Figure 6 shows the results.
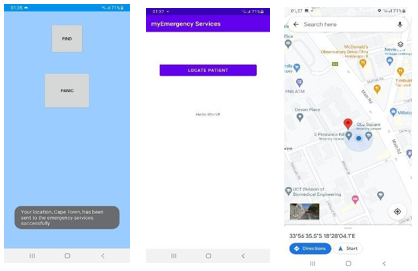
The location of the patient is sent to emergency services via a cloud message. Emergency services retrieve the location and direct to Google Map to show the patient's location.
The device tracks within the range zero to 15 meters. The integration of a buzzer improved fast-locating ability. However, the distance approximation is less robust. False triggers (of being far) were observed and needed improvement. The geolocation was accurate, however, real-time cloud notifications to emergency services were not fully working.
The author would like to acknowledge the University of Cape Town, Medical Devices Lab staff for the assistance during the development of this device. More importantly, the author appreciates the support from Impulse Biomedical for funding the study.
Birgitta, B., Thomas, L., & Dietrich, H. S. (1999). Community Noise. Stockholm University and Karolinska Institute. Retrieved from World Health Organisation: https://www.who.int/docstore/peh/noise/Com noise-4.pdf
Levin, M. E., Risenga, S. M., Kriel, M., Karabus, S., Manjra, A. I., Gray, C. L.,Spuy, D. A. (2015). Severe food allergy and anaphylaxis: Treatment, risk assessment and risk reduction. South African Medical Journal, 72-73. DOI:10.7196/SAMJ.9099
Posner, L., & CA, C. (2017). Update on the usage and safety of epinephrine auto-injectors, 2017. Dovepress, 9-18. DOI:10.2147/DHPS.S121733
Potera, C. (2015). Misuse of Autoinjectors and Inhalers. AJN, American Journal of Nursing, 115(3), 17. DOI:10.1097/01.naj.0000461799.44904.d3
Pumphrey, R. (2004). Anaphylaxis: can we tell who is at risk of a fatal reaction?. Current Opinion In Allergy & Clinical Immunology, 4(4), 285-290. DOI:10.1097/01.all.0000136762.89313.0b
Sheikh, A., Sheikh, A., Simons, F., Barbour, V., & Worth, A. (2012). Adrenaline auto-injectors for the treatment of anaphylaxis with and without cardiovascular collapse in the community. Cochrane Database of Systematic Reviews. DOI:10.1002/14651858.cd008935.pub2