


Alexander Francis, Doron Joffe, Lan Xu, Neil Stacey, David Rubin
ORCID ID: 0000-0003-0729-3750, 0000-0003-1953-9420, 0000-0003-1342-4710,
0000-0003-4902-5201, 0000-0003-0316-9197
School of Chemical Engineering
University of Witwatersrand
Gauteng
South Africa
Previous research has demonstrated the viability of kidney dialysers repurposed as extra-corporeal membrane oxygenation devices to provide sufficient supplemental oxygen support for those suffering from COVID-19. This study focused on determining the mass transfer coefficient for carbon dioxide in kidney dialyser cartridges at varying pH levels. CO2 mass transfer coefficients of 5.5 and 6.95 𝑚𝑔/𝑘𝑝𝑎∙𝑚𝑖𝑛 were achieved, depending on the type of hollow fibre membrane dialyser — this corresponds to a CO2 removal rate of between of 80% and 90% of the total CO2 produced by the body. The mass transfer coefficients achieved with water as the medium suggest that sufficient CO2 removal for respiratory requirements can be achieved with hollow fibre membrane dialysers. This should motivate further experimentation with blood to determine the feasibility of using the cost-effective hollow fibre membrane dialysers to supplement conventional extra-corporeal membrane oxygenation technologies in resource-constrained hospital wards. It is also found that hollow fibre membrane dialysers have high sieving coefficients for dissolved ions, which indicates that dissolved solids and plasma ions will leak from the cartridge and supplements will need to be given to patients to account for these losses. The sieving coefficient for the kidney dialyser cartridge was calculated to be an average of 0.983. The results in this study are promising, adding additional parameters to the body of knowledge for devising operational protocols. However, more specific experimentation using blood is warranted.
Keywords: COVID-19; Respiratory Support, Emergency healthcare capacity
| ECMO | Extra-Corporeal Membrane Oxygenation |
| HFMD | Hollow Fibre Membrane Dialyse |
The COVID-19 pandemic has resulted in millions of deaths and many more infections. It may also cause long-term lung injury in those who survive — with pneumonia and respiratory-failure being the main causes of mortality. As COVID-19 affects countries in waves, oxygen treatment is at its highest demand near the peak of each wave. In extreme cases, the demand is unable to be met due to a lack of supplemental oxygen treatment devices.
Both ECMO and HFMDs operate through diffusion of solutes to and from the patient’s blood stream. It has been suggested to repurpose renal hollow fibre membrane dialysers as ECMO machines to reduce the shortfall of supplemental oxygen treatment devices (Rubin et al, 2020). There are many risks involved with the use of an ECMO device. Primarily, a safe ECMO device must concomitantly oxygenate and decarbonate blood to appropriate levels in a patient with respiratory distress. The mass transfer characteristics for carbon dioxide in hollow fibre membrane dialyser cartridges need to be investigated to assess the suitability of the cartridges as a possible treatment option for patients suffering from respiratory distress during resource scarce situations. The hollow fibre membrane dialyser needs to transfer sufficient oxygen into the blood to prevent or limit hypoxia and hypoxemia. Additionally, excessive carbon dioxide removal from the blood can result in hypocapnia, while insufficient carbon dioxide removal can result in hypercapnia.
The goal of ECMO is to maintain the patient’s blood oxygen saturation at a minimum of 90% and between 92% - 95% for pregnant women while simultaneously maintaining healthy CO2 levels in the blood (Whittle, Pavlov, Sacchetti, Atwood & Rosenberg, 2020). Healthy blood oxygen levels are at 95% saturation and above (Davis, 2021). This is in contrast to patients suffering from COVID-19 where blood oxygen saturation as low as 50% has been observed (Loyola Medicine, 2020).
Once the disease processes associated with COVID-19 infection have reduced a patient’s oxygen levels, the patient will begin to take deeper and quicker breaths. This exacerbates the inflammatory response and unintentionally causes lung damage. At this stage, the patient is still expelling CO2 and will not feel discomfort because the blood is still at normal pH levels. Chemical feedback from CO2 levels in the blood, rather than O2 levels, governs the respiratory drive, which is why patients do not experience discomfort (Leusen, 1953; Epstein et al., 1995; Vaporidi et al., 2020). Tissue damage worsens over time as the patient unwittingly suffers from dangerously low oxygen levels (PaO2 > 60mmHg) until hospitalisation is required (Dhont, Derom, Van Braeckel, Depuydt & Lambrecht, 2020; Tobin, Laghi & Jubran, 2020). The patient will eventually develop hypercapnia which results in dyspnoea (Zubieta-Calleja & Zubieta-DeUrioste, 2020). Once a patient is hospitalised, it is crucial to implement oxygen therapy before the patient becomes critically ill.
A vital parameter of any ECMO application is the gas transfer rate that can be achieved to and from the patient’s blood stream. A membrane with high resistance to mass transfer will be inadequate to meet oxygenation requirements and adequate quantities of CO2 will not be removed. Conversely, excessive gas transfer may lead to the onset of hypocapnia where the blood CO2 levels drop below the normal reference range of 35 mmHg (Sharma and Hashmi, 2021). Experimental precedent exists for successfully using a low-flux hollow fibre dialyser with a polysulfone membrane to achieve oxygen transfer rates of approximately 37.5 ml/min at a blood flow rate of 500ml/min (Rubin et al., 2020). It has been suggested that using two dialysis devices in parallel could provide up to 75ml/min (Rubin et al., 2020). Although this would not satisfy a critically ill patient’s oxygen requirement, it would be useful for patients with some breathing capability as a means of compensating for a respiratory deficit.
Only a fraction of a patient’s regular O2 supply needs to be recovered to counter the adverse effects of hypoxia. Therefore, (Rubin et al., 2020) proposed using hollow fibre membrane dialysers to meet the demand for supplemental oxygen. This is because haemodialysis cartridges are in abundance and can supply limited respiratory support. If the mass transfer properties of oxygen and carbon dioxide of the dialyser are known, there is potential for hollow fibre membrane dialysers to be used in the place of ECMO machines because they are cheaper and are medical grade. The high rate of hospitalisation of COVID-19 patients has led to shortages of respiratory support equipment in certain regions of the world (Kliff et al., 2020). Substituting ECMO machines for hollow fibre membrane dialysers could have a significant impact in Africa, where resources and medical equipment are scarce.
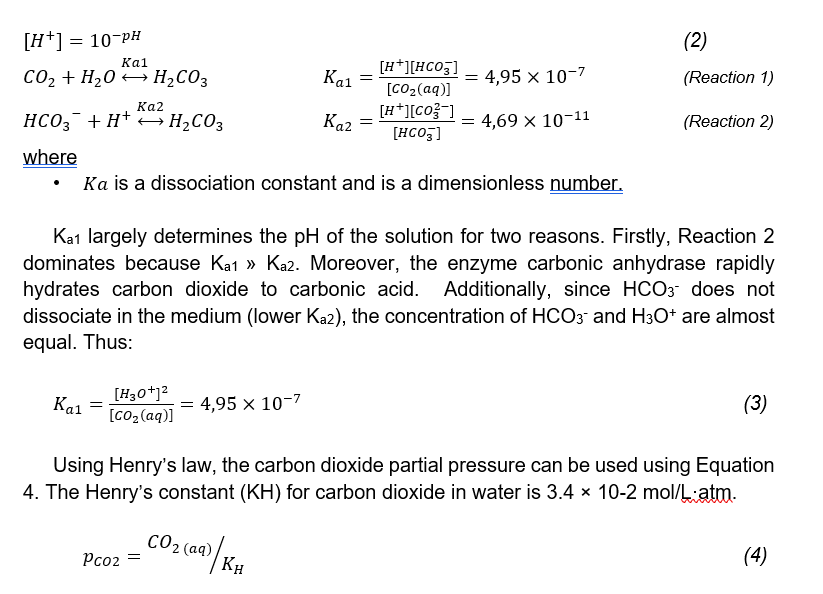
Seventy per cent of carbon dioxide in blood is transported through a series of catalysed acid base reactions involving carbonic acid, bicarbonate, and hydrogen ions. The remainder of carbon dioxide transport is facilitated by carbaminohaemoglobin (23%) and dissolution in plasma (7%) (Biga et al., 2020). The acid-base relationships are defined in Reaction 1 and Reaction 2. Reaction 1 is catalysed by the enzyme carbonic anhydrase (Biga et al., 2020).
A process known as oxygenator wetting can occur where blood plasma infiltrates the membrane micropores and inhibits gas transfer (Yeager and Roy, 2017). Oxygen transfers far less rapidly through water than air and thus, the ECMO functionality is compromised (Yeager and Roy, 2017). Blood products would need to be replenished in the patient’s blood stream via blood transfusion or a drip. The extent of leakage of dissolved solids and ions from the cartridge can be numerically quantified through the sieving coefficient. The coefficient describes the relationship between the concentration of the fluid at the membrane inlet and the concentration of the filtrate (Hulko et al., 2018). It can be used to predict solute loss in blood. A coefficient of one indicates that the solute passes freely through the membrane (Hulko et al., 2018). This is a vital parameter because it indicates the extent to which blood products need to be replaced via a drip or blood transfusion to supplement for solute losses.
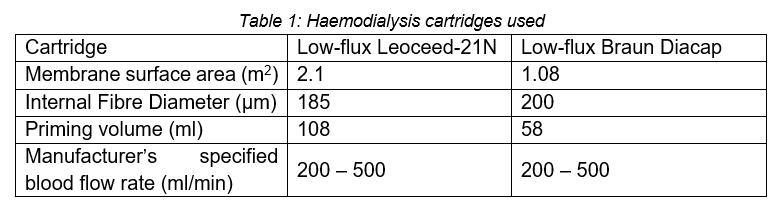
The aim of this study was to determine the mass transfer coefficient for carbon dioxide in water at varying pH levels for the two haemodialysis cartridges shown in Table 1. This will indicate whether the cartridges can remove sufficient carbon dioxide and their viability as makeshift ECMO devices can be assessed. Additionally, this study aimed to determine the sieving coefficient of the cartridges. Both parameters are necessary for developing a clinical plan for implementation of emergency repurposing of HFMDs as makeshift ECMO devices. The sieving coefficients for dissolved solids and ions will indicate the rate at which blood products will have to be replaced in a patient undergoing treatment. For the proposed treatment to be viable, the removal rate of CO2 must be adequate to support respiration. However, in the situation where the CO2 removal rate is excessively high, some amount of CO2 will need to be added to the oxygen stream to maintain normal CO2 levels in the blood.
The experiments were performed at a laboratory in Johannesburg, at an altitude of 1 750m with an atmospheric pressure of about 84kPa and a temperature of about 28°C during the course of experimentation.
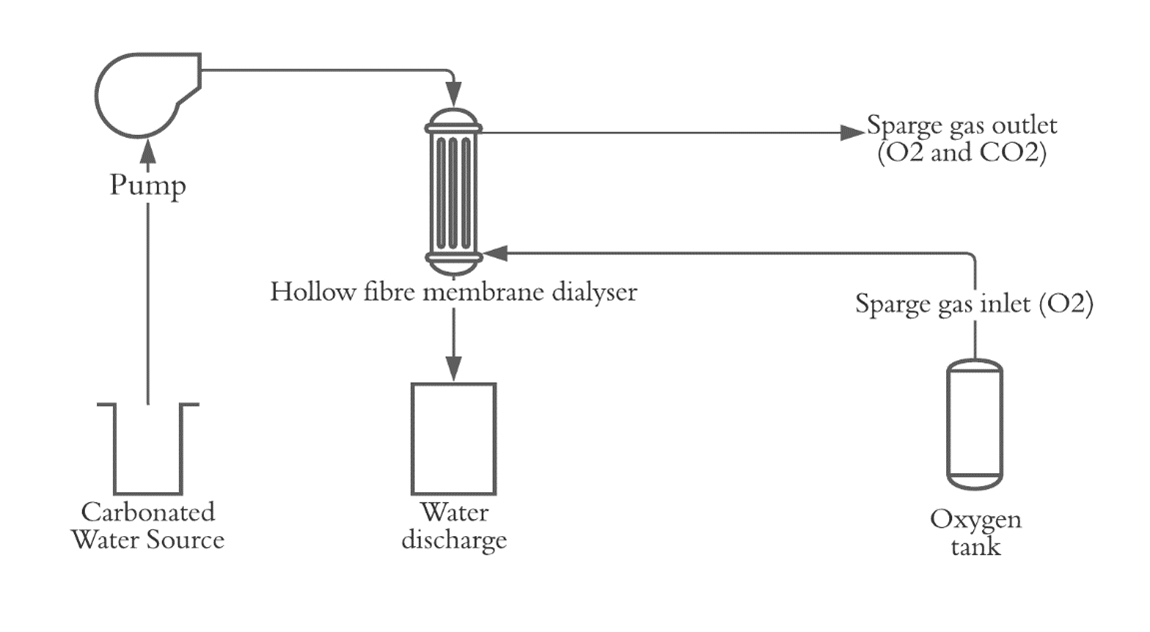
To determine the mass transfer coefficient, carbonated water needed to be pumped counter current to a pure oxygen stream through the cartridge. Carbonation of distilled water was done using a canister of high-pressure CO2, followed by dilution to reach the target pH. The water was pumped at a rate of 500ml/L and the oxygen sweep gas flowed at a rate of 1.5L/min. The pH of the water source was measured as well as the pH of the water after discharge. Subsequent to discharge, the water was diluted by a factor of five and reused as the carbonated water source for the next run. The cycle was repeated until the pH of the water remained unchanged after running through the cartridge. This indicated that an equilibrium had been reached and no further gas transfer was possible. To ensure experimental accuracy, prior to each run, the circuit was primed with twice the recommended priming volume of the cartridge.
The experimental procedure to determine the sieving coefficient was similar. Table salt was added to distilled water to produce the water source. The dissolved solids concentration was measured instead of the pH. The properties of the two types of haemodialysis cartridges used are shown in Table 1. These cartridge types were selected because it has previously been found that high-flux cartridges exhibit high rates of leakage when operated with a gas stream making them unsuitable for this purpose (Xu, 2020).
The mass transfer coefficient can be found using Equation 1, which is derived from Fick’s law. The driving force for carbon dioxide transfer is the partial pressure difference of carbon dioxide across the membrane
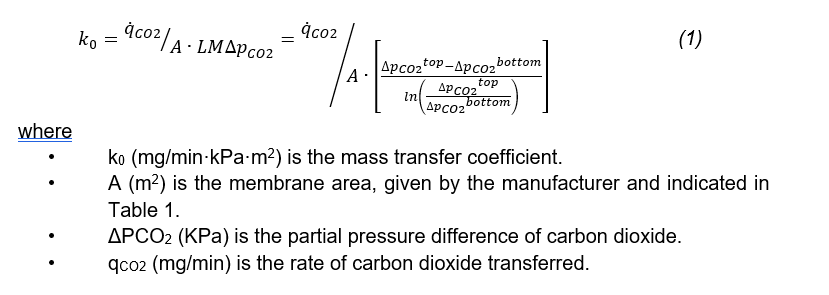
The relationship between carbonic acid and water can be used to calculate the carbon dioxide concentration difference between the water source and discharge. It can further be used to determine the partial pressure of carbon dioxide. The concentration of hydrogen ions in the water can be calculated using Equation 2
When pure oxygen is used as the sweep gas and enters from the bottom, the partial pressure of carbon dioxide in the sweep gas is zero and thus ΔpCO2, bottom = PaCO2 out, liquid. At the top, carbon dioxide in the liquid transfers through the membrane into the gas. The carbon dioxide present in the gas outlet is calculated by doing a mass balance on the carbon dioxide over the liquid inlet and outlet. The partial pressure of carbon dioxide in the gas outlet can then be calculated. The partial pressure difference at the top is taken as the difference between the partial pressure of carbon dioxide in the liquid inlet and gas outlet streams.
The rate of carbon dioxide passing the membrane (qCO2) is found using the pH measurements. The number of H+ ions can be determined by Equation 2. The aqueous CO2 concentration (mol/l) can be found using the acid-base equilibrium constant described by Equation 3, appropriate unit conversion to mg/m3 must be made.
The extent of leakage of dissolved solids and ions from the cartridge can be numerically quantified through the sieving coefficient, defined in Equation 5 below. The electrical conductivity (EC) of the solution gives an indication of the concentration of dissolved plasma ions. The ratio between the EC of the solution before and after passing through the cartridge membrane indicates the extent of the leakage of dissolved ions
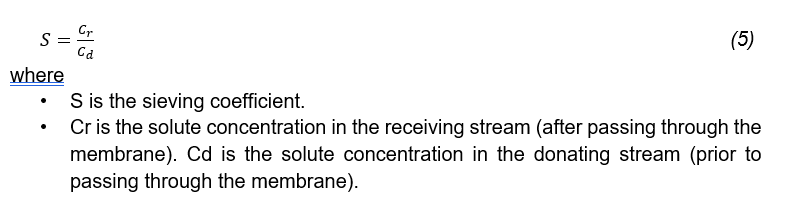
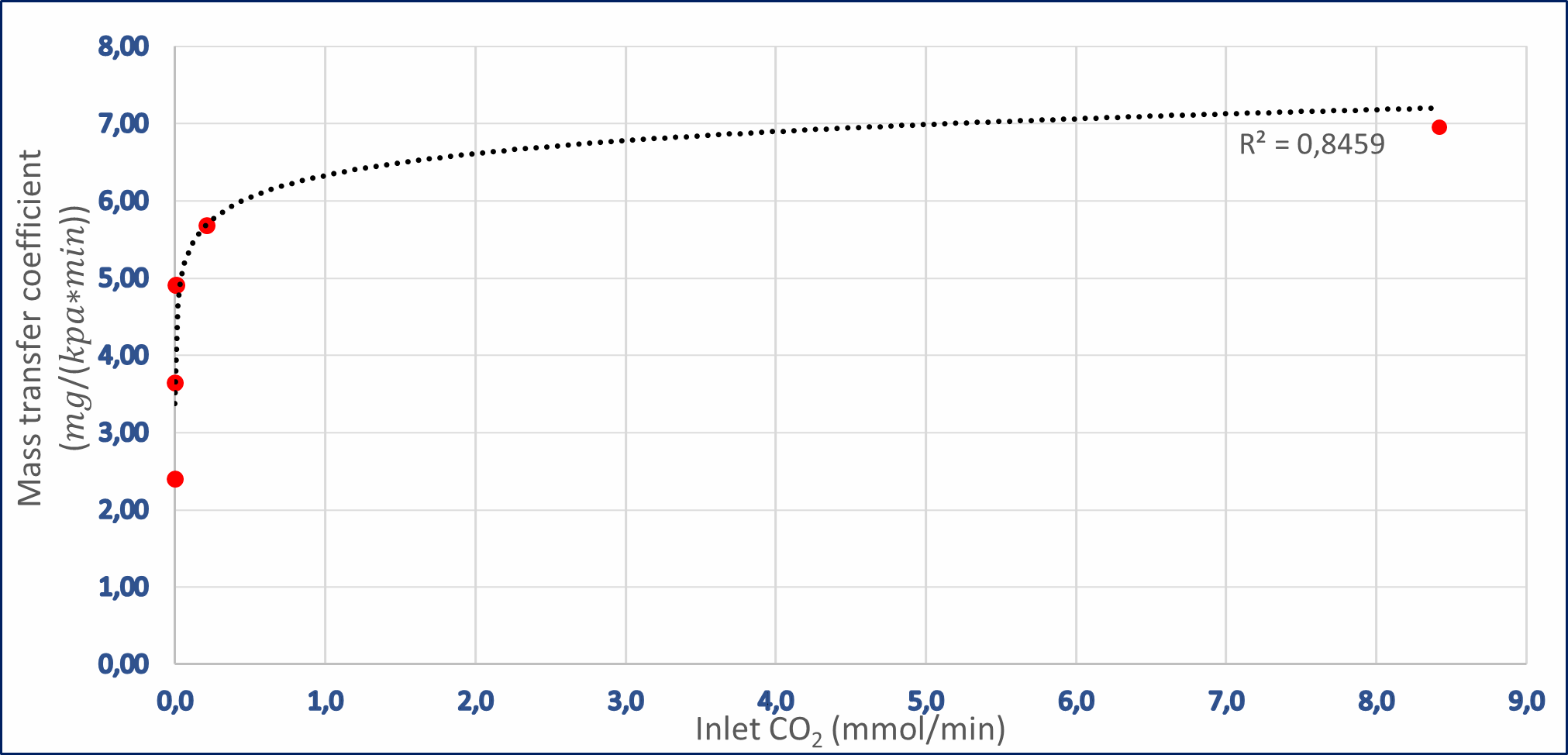
The mass transfer coefficients for both cartridges were calculated. Maximum mass transfer coefficients of 6.95 𝑚𝑔/𝑘𝑝𝑎∗𝑚𝑖𝑛 and 5.5 𝑚𝑔/𝑘𝑝𝑎∗𝑚𝑖𝑛 were obtained in the Braun and Leoceed cartridges, at CO2 inlet concentrations of 8.5 mmol/L and 5.6 mmol/L, respectively.
As shown in Figures 2 and 3, the relationship between the mass transfer coefficient and the inlet CO2 coefficient fits a logarithmic profile with R2 values of 0.85 and 0.92 for the Braun and Leoceed cartridges respectively. The relatively high R2 values indicate that the logarithmic trendlines fit the data points relatively accurately and can be used to forecast values at inlet concentrations that were not tested.
It is evident that the mass transfer coefficient for both cartridges is strongly dependent on the inlet CO2 concentration, but mass transfer coefficients are typically dependent on the membrane material and the type of transporting medium, not inlet concentrations. The apparent dependence on concentration may indicate that there is a two-step process taking place during the dialysis procedure. There could be a reactive equilibrium in the liquid followed by mass transfer through the membrane. Higher CO2 inlet concentrations will increase the rate of the forward reaction in the reactive equilibrium and subsequently increase the apparent overall mass transfer coefficient. This phenomenon merits further study in experiments purpose-designed to examine it, as its presence suggests that CO2 dissolution/diffusion systems may be more accurately considered to be a multi-reaction equilibrium system.
The trendlines show an x-axis asymptote occurs when the carbonated water has reached an equilibrium — no further CO2 removal from the liquid is possible. The y-axis asymptote represents the maximum possible mass transfer coefficient of the cartridge. The x-axis asymptote for the Braun cartridge occurs at a CO2 concentration of approximately 7.33×10-4 mmol/L (corresponding pH ≈ 6.22). The y-axis asymptote for the Braun cartridge is at the maximum transfer coefficient value previously reported. Experiments conducted with the Leoceed cartridge did not use inlet concentrations near the asymptote points; therefore, the exact asymptote values cannot be accurately reported. However, the logarithmic trendline suggests that the values will be similar to those of the Braun cartridge.
The Braun and Leoceed cartridges were tested at dissimilar ranges of inlet CO2 concentrations. However, by using the logarithmic trendlines to extrapolate values at inlet concentrations that were not tested, it can be determined that, on average, the Braun cartridge has a higher overall mass transfer coefficient for each respective CO2 inlet concentration. This is counterintuitive because the Braun cartridge has a lower surface area than the Leoceed cartridge. Subsequently, the Braun cartridge should have a lower overall mass transfer coefficient. Thus, further experimentation is needed to obtain more data points and eliminate the need for extrapolating trend lines.
Similar results were found in literature for experiments that have been conducted on a Leoceed cartridge. However, the liquid that was used in those experiments was blood (Rubin et al., 2020). If the logarithmic profile for the Leoceed cartridge is extrapolated to match the inlet concentration that was used in the literature experiments, Figure 3 indicates the literature values are slightly higher than the experimental values. This is expected because in blood the CO2 conversion to the bicarbonate ion is catalysed by the enzyme carbonic anhydrase. Therefore, the reaction rate producing hydronium and bicarbonate ions will always be higher in blood than in water, which would be expected to result in a higher apparent mass transfer coefficient in blood than in water.
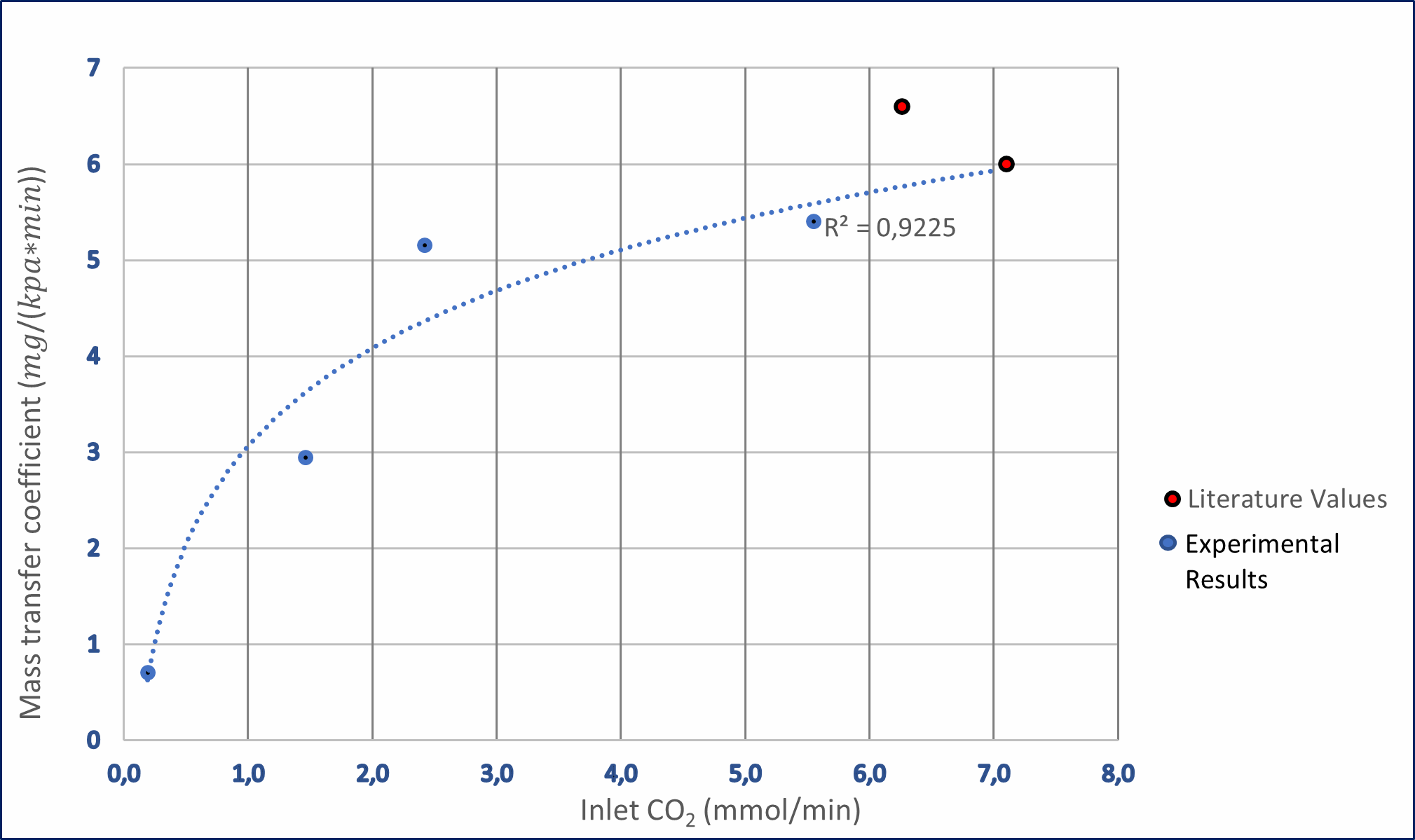
The volume of CO2 that can be removed from the liquid each minute can be calculated based on the calculated mass transfer coefficients. In Figure 4 the relationship between CO2 transferred cross the membrane and the water inlet CO2 concentration is shown. For both cartridges the trend is linear and the equation of the line of best fit for the Braun cartridge is y = 0.725x - 0.0035 with an R2 value of 1 while the equation for the Leoceed cartridge is y = 0.6449x - 0.0879 with an R2 value of 0.9988. The high R2 values for both graphs indicate that the data points are clustered close enough that both functions can be deemed valid to approximate the data.
To determine whether sufficient carbon dioxide is removed by the cartridge, the difference in the carbon dioxide content in the arteries and veins in the human body must be known. The arteries carry oxygenated blood that has a lower carbon dioxide content relative to the de-oxygenated blood found in veins. The concentration of carbon dioxide in arterial blood is 21.5mmol/L compared to 23.5 mmol/L in venous blood (Arthurs & Sudhakar, 2005). The difference in the carbon dioxide content between the venous and arterial blood is thus only 2mmol/L. The aim should be to remove this amount of CO2 from the blood because excessive removal can lead to hypocapnia in the patient. Insufficient removal can result in accumulation of carbon dioxide in the blood, and the subsequent onset of hypercapnia in the patient.
Both cartridges remove too much carbon dioxide and are projected to remove as much as 16mmol/L of carbon dioxide from the water at a carbon dioxide concentration similar to that found in venous blood. Such excessive removal of carbon dioxide would be detrimental to a patient’s health. However, this problem can be solved easily. The amount of carbon dioxide transferred across the membrane can be reduced by increasing the carbon dioxide content in the sweep gas. Consequently, the driving force for mass transfer of carbon dioxide across the membrane will be reduced and the aim of reducing the carbon dioxide concentration in the blood by only 2mmol/L can be achieved. COVID-19 patients frequently exhibit so-called 'silent hypoxia', a condition where SpO2 is reduced without elevated CO2 levels and discomfort typically associated with respiratory distress. Consequently, it can be argued that removing additional CO2 is not necessarily desirable in many COVID-19 patients.
The “distilled water” provided for the experimentations had pH levels slightly below six. This suggests a presence of ions which may have detrimentally affected the results. The mass transfer coefficient for carbon dioxide in water in both cartridges is deemed sufficiently large to remove enough carbon dioxide from blood. However, adjustments will need to be made to the sweep gas to reach the target of removing 2mmol/L of carbon dioxide from venous blood. The mass transfer coefficient results highlight the potential of the technology and warrant further research on human blood (as opposed to water). The results from this study are not directly comparable to those that would be obtained through the use of blood, although they can be used to make a fair estimation.
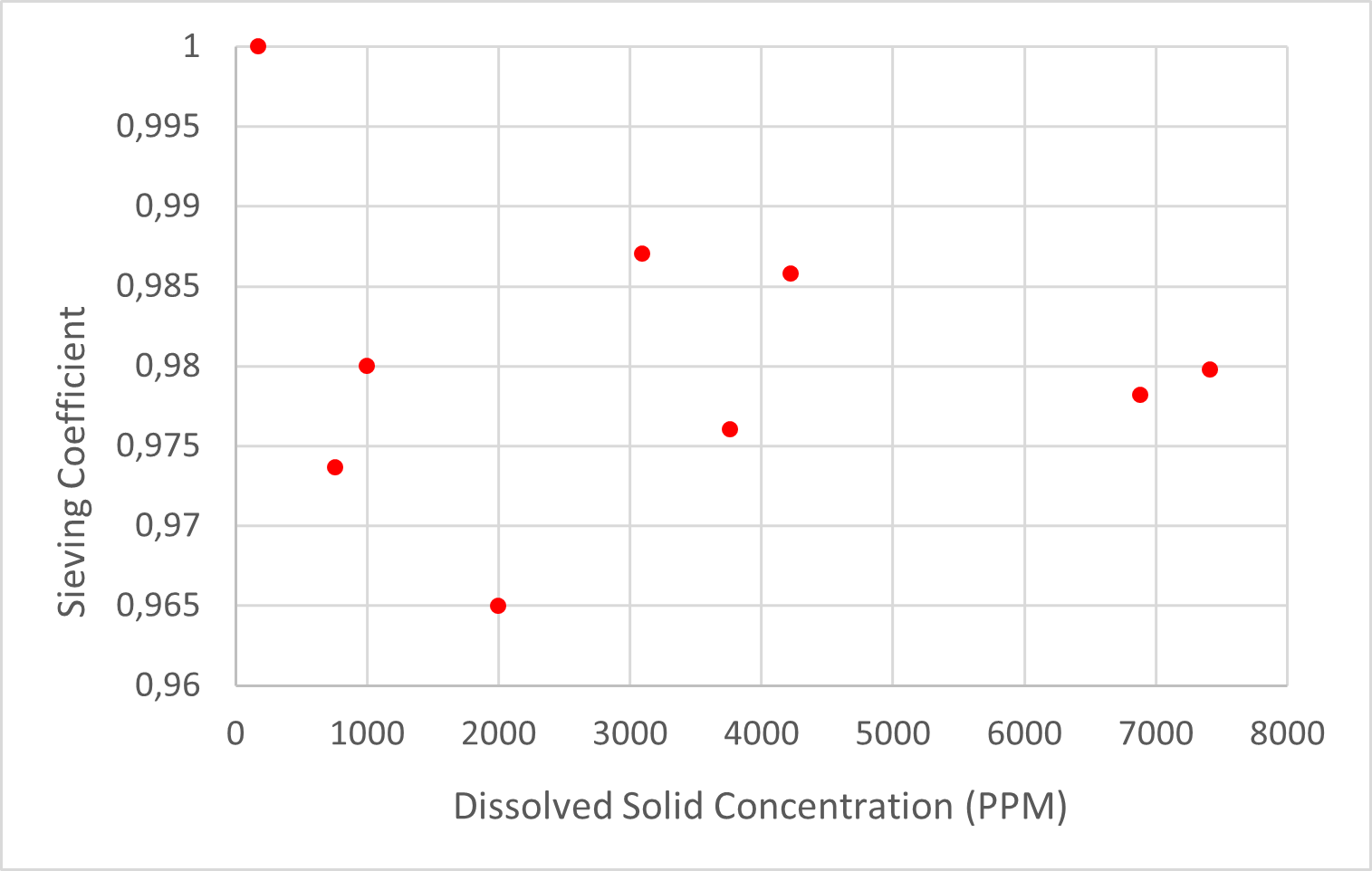
Sieving coefficients were calculated at various dissolved solid inlet concentrations. The results plotted in Figure 5 below indicate that the sieving coefficient for the Braun dialysis cartridge fluctuates around 0.98. There is no trend in the sieving coefficient and the dissolved solids concentration has no effect on the sieving coefficient. This indicates that the sieving coefficient is independent of the original dissolved solids concentration.
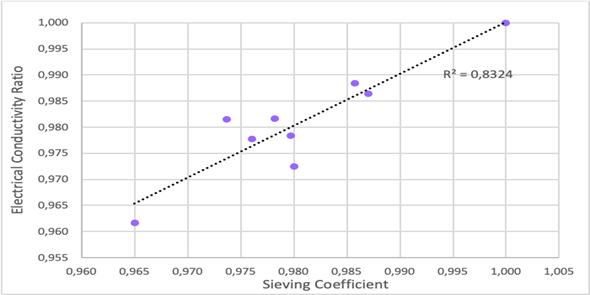
The electrical conductivity of the solution was measured alongside the dissolved solids concentration and the ratio of the electrical conductivity between the source and discharge was calculated. The average electrical conductivity ratio was 0.981 and was also unaffected by the varying levels of dissolved solids concentration. The electrical conductivity ratio was plotted against the sieving coefficient and a change in one of them led to a proportional change in the other. This is shown in Figure 6, and it validates the data collected during the experimentation, as one would expect the dissolved solids and electrical conductivity of the solution to decrease or increase proportionally. The loss of ions and dissolved solids can be attributed to accumulation inside the cartridge and the leakage that occurs.
About 2% of the dissolved solids and ions in the water is lost when passing through the dialysis cartridge. In practice, when operating on a patient, there will be about a 2% loss in the blood products for each time the patients' entire blood volume passes through the cartridge. This a significant loss in blood products considering that some patients suffering from COVID-19 require oxygen therapy over a period of days and possibly weeks. If this method is to be used, the patient may require a drip or blood transfusion to supplement the loss of blood products.
The mass transfer coefficient for CO2 permeating the hollow fibre membrane dialysers exceeds the minimum target for adequate CO2 removal. This initially suggests the feasibility of the technology. However, some uncertainty about this result remains because the mass transfer coefficient was not constant over the range of pH levels at which it was tested. This is inconsistent with linear Fick’s Law behaviour. This could indicate that a two-step process occurs such that a reactive equilibrium in the liquid occurs followed by the transfer of carbon dioxide through the membrane. This casts some doubt on the direct applicability of this result when operating with blood, because the liquid-phase reactions will have different reaction kinetics in blood. The haemodialysis cartridges have the potential to be used as a makeshift ECMO device in a resource constrained setting.
The sieving coefficient for the dissolved ions tested was calculated as 0.983, which suggests that those ions pass freely through the membrane material along with the solvent. This suggests there will be about a 1.7% loss in water-soluble blood products every time a patient’s total blood volume is pumped through the cartridge, based on the observed leakage rates. These losses will have to be replaced, most likely intravenously. The results from this study are promising, but further experimentation using blood is required to determine mass transfer coefficients more accurately.
The authors would like to acknowledge the funding from merSETA provided by the MediVentors Consortium and the laboratory space and equipment provided by Wits University.
Biga, L., Harwell, A., Hopkins, R., Kaufmann, J., LeMaster, M., Matern, P., & Morrison-Graham, K. (2020). Transport of Gases. In L. Biga, S. Dawson, A. Harwell, R. Hopkins, J. Kaufmann & M. LeMaster et al., Anatomy and Physiology (1st ed.). Oregon State University. Retrieved from https://open.oregonstate.education/aandp/chapter/22-5-transport-of-gases/
Davis, C. (2021). Safe, Normal, Low Blood Oxygen Levels: Pulse Oximeter Chart. Retrieved 26 September 2021, from https://www.onhealth.com/content/1/normal_low_blood_oxygen_pulse_oximeter_lev els
Dhont, S., Derom, E., Van Braeckel, E., Depuydt, P., & Lambrecht, B. (2020). The pathophysiology of ‘happy’ hypoxemia in COVID-19. Respiratory Research, 21(1). doi: 10.1186/s12931-020-01462-5
Hulko, M., Haug, U., Gauss, J., Boschetti-de-Fierro, A., Beck, W., & Krause, B. (2018). Requirements and Pitfalls of Dialyzer Sieving Coefficients Comparisons. Artificial Organs, 42(12), 1164-1173. doi: 10.1111/aor.13278
Kliff, S., Satariano, A., Silver-Greenberg, J. and Kulish, N. (2020). There Aren’t Enough Ventilators to Cope with the Coronavirus. Retrieved 17 November 2021, from https://www.nytimes.com/2020/03/18/business/coronavirusventilatorshortage. html
Leusen, I. (1953). Chemosensitivity of the Respiratory Center. American Journal Of Physiology-Legacy Content, 176(1), 39-44. doi: 10.1152/ajplegacy.1953.176.1.39
Rubin, D., Stacey, N., Matambo, T., Vale, C., Sussman, M., & Snyman, T. et al. (2020). Toward Respiratory Support of Critically Ill COVID-19 Patients Using Repurposed Kidney Hollow Fiber Membrane Dialysers to Oxygenate the Blood. Journal Of Healthcare Engineering, 2020, 1-6. doi: 10.1155/2020/8862645
Tobin, M., Laghi, F., & Jubran, A. (2020). Why COVID-19 Silent Hypoxemia Is Baffling to Physicians. American Journal Of Respiratory And Critical Care Medicine, 202(3), 356-360. doi: 10.1164/rccm.202006-2157cp
Vaporidi, K., Akoumianaki, E., Telias, I., Goligher, E., Brochard, L., & Georgopoulos, D. (2020). Respiratory Drive in Critically Ill Patients. Pathophysiology and Clinical Implications. American Journal Of Respiratory And Critical Care Medicine, 201(1), 20-32. doi: 10.1164/rccm.201903-0596so
Whittle, J., Pavlov, I., Sacchetti, A., Atwood, C., & Rosenberg, M. (2020). Respiratory support for adult patients with COVID-19. Journal Of The American College Of Emergency Physicians Open, 1(2), 95-101. doi: 10.1002/emp2.12071
Loyola Medicine. (2020). Hypoxia Covid. Retrieved 17 November 2021, from https://www.loyolamedicine.org/about-us/news/new-study-explains-potentialcausesfor- happy-hypoxia-condition-in-patients-with-the-covid19-virus
Xu, L., 2020. Hollow Fiber Membrane Dialysers: Gas transfer properties of Hollow Fibre Membrane Dialysers repurposed for respiratory support in critically ill COVID-19 patients. doi: 10.13140/RG.2.2.33285.83680
Zubieta-Calleja, G., & Zubieta-DeUrioste, N. (2020). Pneumolysis and “Silent Hypoxemia” in COVID- 19. Indian Journal Of Clinical Biochemistry, 36(1), 112- 116. doi: 10.1007/s12291-020-00935-0