


Lara Timm, Maureen Etuket, Sudesh Sivarasu
ORCID ID: 0000-0003-2073-9649, 0000-0002-9581-3762, 0000-0002-0812-568X
University of Cape Town
Cape Town
South Africa
Presently, open-source prosthesis is not optimised to assist the dominant hand in performing bimanual ADL. This research study was thus geared towards the design and experimental validation of an open-source below-elbow prosthetic arm, called the ADL arm, that is functionally optimised for the performance of ADL in the unilateral trans-radial (TR) amputee population. The ADL arm is 3D printed; the design validation involved functional assessment - using the AHAP and simulated use assessment with healthy volunteer participants after obtaining Ethics approval. In accordance with AHAP, the ADL arm presented with an overall GAS of 68% and a partial GAS of >75 % for 4/5 ADL grasps. Usability Assessment involved the performance of ADL tasks coupled with the completion of the SUS. The perceived usability of the device was found to increase with increased device familiarity, yielding an overall score of 84.29. Through the tests conducted, the ADL arm was found to be functionally competent, relatively acceptable with proven ability to assist in the performance of ADLs in a simulated-use environment. A number of design modifications and clinical tests are however recommended to overcome the limitations of the current design and corroborate the results obtained in this study.
Keywords: Open source; Prosthesis; Trans-radial
| ADL | Activities Of Daily Living |
| AHAP | Anthropomorphic Hand Assessment Protocol |
| CC | Creative-Common |
| FDM | Fused Deposition Modelling |
| GAS | Grasping Ability Score |
| IADL | Instrumental Activities of Daily Living |
| OT | Orthopaedic Technician |
| ROM | Range of Motion |
| TR | Trans-radial |
| TD | Terminal Device |
TR amputation is traumatic, leading to the amputee having a limited ability to perform activities of daily living (ADLs) like eating, dressing, toileting, grooming and ambulation (Pasquina, Cooper & Lenhart, 2009). Below-elbow prostheses are hence prescribed. TR- (below- elbow) amputation refers to the partial removal of the upper limb between the elbow and wrist joints. Such amputations are performed for various reasons, including irreparable physical trauma, certain diseases, and birth defects (Ovadia & Askari, 2015; Jette, Spicer & Flaubert, 2017). The incidence of upper-limb amputations in South Africa (SA) is not well documented. As of 2020, there are approximately 11 000 major upper extremity amputees living in SA, where major amputations exclude amputations more distal than wrist level (Ziegler-Graham, MacKenzie, Ephraim, Travison & Brookmeyer, 2008).
In most scenarios, prosthetic intervention forms part of the post-surgical rehabilitative pathway for below-elbow amputees (Saradjian, Thompson & Datta, 2008). The high cost associated with prostheses, however, results in many amputees in low-to-middle income countries relying on government subsidized devices, which are cosmetic rather than functional, or none at all. Functional prostheses are preferred to their cosmetic counterparts as they allow for a wide range of varied motion hence supporting both the primary and secondary goals that make up the ADLs (Jette, Spicer & Flaubert, 2017; Østlie et al., 2012).
Open-source prostheses, made possible by the internet, are aimed at improving device accessibility, reducing device costs, encouraging collaborative design and a sustainable value chain (Alami et al., 2020). However, the open-source prosthetic arms that are currently available have two main goals: to be an inexpensive solution for child amputees who outgrow prostheses very quickly, or to replicate electric arm prostheses in an inexpensive and accessible manner (Alami et al., 2020; Enabling The Future, 2021).
Currently, a body-powered prosthetic arm intended to assist the dominant hand of a unilateral amputee in performing ADLs does not exist. By increasing personal autonomy, such a device would greatly benefit adult amputees in LMICs who do not have access to functional prostheses. Hence, this study focused on the development of a functional below- elbow prosthetic arm (the ADL arm) that is optimised to assist in the performance of bimanual ADLs. The ADL arm is designed to reliably perform the grasps required by the non-dominant hand in two handed ADL activities. Further, the study aims at validating the functionality and efficacy of the ADL arm by conducting functional and simulated-use testing.
The ADL arm Prototype 1 was developed by selecting and combining favourable components of existing open-source designs available in the CC space and designing novel components to achieve a solution functionally optimised for the performance of bimanual ADLs as summarised in Table 1.
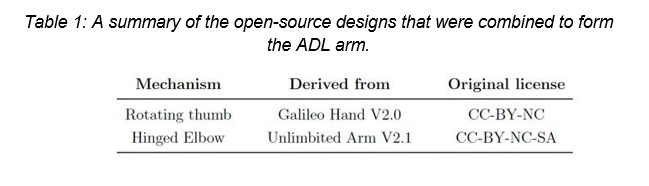
This ADL arm uses torque generated by flexion of the elbow joint to actuate the hand TD. The prosthesis is suspended using Velcro straps that secure the device to the biceps and forearm of the amputee as shown in Figure 1. These straps allow for easy adjustment to fit different users. Customisability is also achieved through 3D printing which allows for improved individual fit, comfort, and level of anthropomorphism (Alami et al., 2020; Gibson & Srinath, 2015).
The hand TD is voluntary closing. Each digit is restored to its resting position by an elastic element. Notable features of the design are the under-actuation mechanism, which facilitates adaptive grasp; the rotating thumb mechanism, which allows adduction and abduction of the thumb; and the rotating wrist mechanism, which allows pronation and supination of the TD.

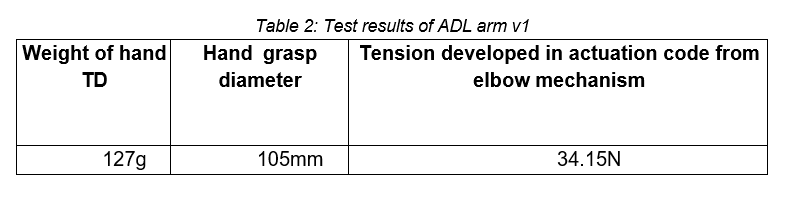
Testing of the ADL arm V1 yielded results shown in Table 2 that led to its further development into a parametric prosthetic arm design that is more suitable for modification and fabrication with limited resources. This process is described in subsequent sections.
The design process began with a consideration of the parameters which affect the overall device efficacy as shown in Figure 2. The initial system parameters were identified by reviewing the available literature, through several discussions with a consulting OT, Michael Awood, and following the results obtained after testing the first prototype (ADL V1).
The system parameters included:
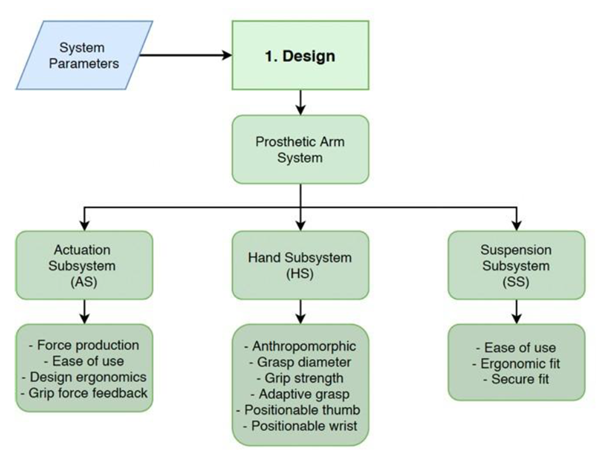
The design of the prosthesis –ADL Arm V2 proceeded with the design and testing of the individual three subsystems: AS, HS and SS shown in Figure 2 and final assembly to form the ADL AMR V2 prototype.
The physical prototype of the ADL arm is an assembly of 3D printed parts and accessible hardware components. All 3D printed parts were fabricated using a Creality Ender 3 FDM printer. FDM printed parts suffer an inherent weakness in planes parallel to the print bed, between layers. Some parts, such as the proximal wrist, were designed as an assembly of smaller components. This was to ensure adequate strength of each part in the appropriate direction and to minimise the amount of required support material during printing.
This device is body-powered, featuring a hand terminal device (TD) with thumb abduction and adduction, and wrist pronation and supination functionality. Elbow flexion of the residual limb is used to actuate the hand TD. The hand TD is composed of five digits: four fingers and a thumb. Each digit features a channel that extends the length of its palmar side to house the actuation cord for that digit. The cord is fixed at the fingertip. Applying tension to the cord flexes the digit; releasing cord tension extends the digit. The digit is extended by the restorative spring elements.
Unlike prototype one, the final prototype implements a cable-lock mechanism as shown in Figure 3. This is advantageous as the device is voluntary closing, implying that elbow flexion must be maintained to keep a grip on the object. A cable lock maintains the grip on an object without requiring sustained physical effort from the user. With a cable lock, objects can be grasped away from the body, increasing an amputee's functional work envelope when wearing the device.

AHAP aims to reliably measure the grasping ability of anthropomorphic hands. In this case, grasping ability is defined as the hand's ability to effectively grasp and maintain a stable grip on an object while the arm moves around (Llop-Harillo, Pérez- González, Starke & Asfour, 2019).
The AHAP protocol consists of 26 tasks and uses 10 grasp types associated with performing ADLs. The results of the protocol reveal: A total Grasping Ability Score (GAS): which quantifies the hand's ability to perform the full set of grasps; A partial GAS: which quantifies the hand's ability to perform each specific grasping task; A qualitative indication of the advantages and disadvantages of the hand, its control mechanism, and its actuation mechanism; A starting point to identify the reasons for failed tasks/grasps. The protocol is designed to identify difficulties experienced with grasping and a classification thereof.
For each of the 26 tasks, a trained operator (the innovator) instructed the participant to carry out each step thrice using the ADL ARM V2. Priority was placed on 11 tasks that are representative of those used by bimanual ADLs. The grasp types that were used as a measure for prosthetic success included medium wrap, adducted thumb, lateral grasp, index finger extension, and non-prehensile.
Of the 11 tasks performed using these grasps, a score of at least one had to be achieved for each of the five grasp types specified. That is to say that at least one object per grasp type, and not necessarily all object variations, must be grasped successfully. If the results met these criteria, the device would be considered a success at this stage. Scores were given in this order: a score of one was given for a successful grasp of the correct grasp type, 0.5 if the grasping posture differed from the specification, and zero if the prosthesis could not grasp the object. The definition of grasp success differs per grasp type, however, a score of 100 % is the best-case scenario and corresponds to functionality and anthropomorphism similar to that of a healthy human hand.
Simulated Use Assessment was completed by seven healthy, right-hand dominant individuals. The designed bypass socket was used for this portion of testing as shown in Figure 4. In the first stage, a self-report questionnaire was used which allowed the innovator to quantify the usefulness of the prosthetic device for performing a range of ADL and IADL tasks.

The questionnaire was designed to measure:
In the second stage, the overall device usability was assessed following the acquisition of ethics approval from the UCT Human Research and Ethics Committee under reference number HREC REF 796:2020. Device usability was assessed using seven healthy participants in the laboratory setting divided into three categories: those with no familiarity with the device; those with theoretical experience with the device; and those who were involved in the testing of prototype one. System usability was scored according to the System Usability Scale (SUS) (Brooke, 1996). The SUS questionnaire provides a quantitative measurement of device usability and user experience.
According to a study conducted by Bangor, Kortum and Miller (2008), the average SUS score is 68, while anything above 68 is considered above average. A 'good' score is one larger than 72:75, an 'excellent' score is larger than 85:58 and the 'best imaginable' score is 100. The obtained SUS will be evaluated against this scale.
The physical and mechanical properties of the ADL ARM V2 were evaluated on a subsystem basis and following through with particular parameters of interest reported in Table 3 below:
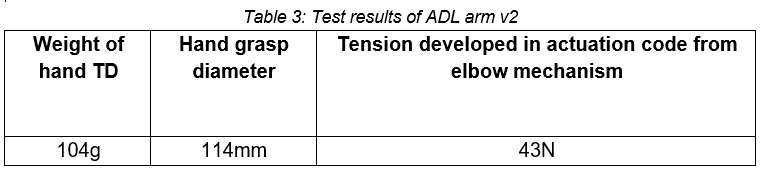
The ROM of the designed TD informs the grasp diameter, and, for the ADL ARM V2, it was comparable to the healthy hand. This achievable ROM allowed the hand to mimic the kinematics of the healthy hand, allowing it to securely grasp objects of a range of sizes, weights, and surface qualities.
The elbow mechanism was able to produce approximately 43 N of tensile force to transmit to the hand. However, this producible tensile force and the grip force measured in the hand were not the same. This may have been due to the shape of the hand TD and the hand grip dynamometer not being suitable for accurate measurement. Another reason for the discrepancy could have been a loss of energy as a result of friction within the digits, or simply that the transmission of cable tension to grip force is not a 1:1 ratio. It also became apparent during testing that the design of the elbow hinge was a limiting factor to how much force the elbow mechanism could produce, calling for further modifications to the elbow hinge and the cable alignment.
The overall GAS and partial GAS of the ADL arm was found to be 68 %. The ADL arm achieved a partial GAS of greater than 75 % for four of five bimanual ADL grasps. A major design flaw resulted in a partial GAS of 33:3 % for the lateral pinch grasp type. The performance in this grasp, as well as others, would be greatly improved by the inclusion of a mechanism to lock the distal joint of the digits in extension during grasp. In this way, the hand would be better able to apply force to an object with the pads of the digits.
The ADL assessment involved the completion of 86 ADL and IADL tasks; scored using the designed self-report questionnaire. The participants could perform all but seven tasks independently, and the perceived difficulty for tasks requiring the prosthesis was low overall.
Participants performed a number of tasks and then completed the SUS. The perceived usability of the device was found to increase with increased device familiarity, yielding an overall score of 84.29. This result indicated that participants found the experience with the device to be 'good' overall.
The ADL arm is functionally competent and has proven its ability to assist in the performance of ADLs in a simulated- use environment, using able-bodied participants. A number of design modifications are recommended to overcome the limitations of the current design, which should be tested in a large TR amputee population to corroborate the results obtained in this study.
Consulting OT: Mr Michael Awood, for his clinical expertise. He provided much insight and advice which made this project possible.
Alami, H., Rivard, L., Lehoux, P., Hoffman, S., Cadeddu, S., & Savoldelli, M. et al. (2020). Artificial intelligence in health care: laying the Foundation for Responsible, sustainable, and inclusive innovation in low- and middle-income countries. Globalization And Health, 16(1). doi: 10.1186/s12992-020-00584-1
Bangor, A., Kortum, P., & Miller, J. (2008). An Empirical Evaluation of the System Usability Scale. International Journal Of Human-Computer Interaction, 24(6), 574-594.doi: 10.1080/10447310802205776
Brooke, J. (1996). Usability Evaluation in Industry (pp. 189-194). Taylor & Francis.
Enabling The Future. (2021). Which Design?. Retrieved 21 October 2021, from https://enablingthefuture.org/which-design/
Gibson, I., & Srinath, A. (2015). Simplifying Medical Additive Manufacturing: Making the Surgeon the Designer. Procedia Technology, 20, 237-242. doi: 10.1016/j.protcy.2015.07.038
Jette, A., Spicer, C., & Flaubert, J. (2017). The promise of assistive technology to enhance activity and work participation. Washington: National Academies Press (US).
Llop-Harillo, I., Pérez-González, A., Starke, J., & Asfour, T. (2019). The Anthropomorphic Hand Assessment Protocol (AHAP). Robotics And Autonomous Systems, 121, 103259. doi: 10.1016/j.robot.2019.103259
Østlie, K., Lesjø, I., Franklin, R., Garfelt, B., Skjeldal, O., & Magnus, P. (2012). Prosthesis use in adult acquired major upper-limb amputees: patterns of wear, prosthetic skills and the actual use of prostheses in activities of daily life. Disability And Rehabilitation: Assistive Technology, 7(6), 479-493. doi: 10.3109/17483107.2011.653296
Ovadia, S., & Askari, M. (2015). Upper Extremity Amputations and Prosthetics. Seminars In Plastic Surgery, 29(01), 055-061. doi: 10.1055/s-0035-1544171
Pasquina, P., Cooper, R., & Lenhart, M. (2009). Care of the Combat Amputee. Washington: TMM Publications.
Saradjian, A., Thompson, A., & Datta, D. (2008). The experience of men using an upper limb prosthesis following amputation: Positive coping and minimizing feeling different. Disability And Rehabilitation, 30(11), 871-883. doi: 10.1080/09638280701427386
Ziegler-Graham, K., MacKenzie, E., Ephraim, P., Travison, T., & Brookmeyer, R. (2008). Estimating the Prevalence of Limb Loss in the United States: 2005 to 2050. Archives Of Physical Medicine And Rehabilitation, 89(3), 422- 429. doi: 10.1016/j.apmr.2007.11.005