Chapter 3:
ENDOCRINE DISORDERS
Student Authors: Lehlohonolo Ntlatlapo and Belene Demeke
This chapter covers the following topics:
- Normal puberty
- Disorders of puberty
- Approach to growth disorders
- Thyroid disorders
- Diabetes mellitus
- Hypoglycaemia
NORMAL PUBERTY
Definition
Puberty is a well-defined sequence of physical and physiological changes which occur during adolescence and culminate in the attainment of full physical and sexual maturity. In addition to physical changes, puberty is accompanied by cognitive and psychological maturation.
Physiology
Puberty is under the control of the hypothalamic-pituitary-gonadal axis. It begins when the hypothalamus starts releasing gonadotropin-releasing hormone (GnRH) into the hypophyseal portal system.
GnRH stimulates the pituitary gland to release the two gonadotropin hormones, luteinising hormone (LH) and follicle-stimulating hormone (FSH). LH and FSH signal the ovaries and testes to release sex hormones (oestrogen in females and testosterone in males), which trigger the maturation of the sex organs and the development of secondary sexual characteristics (SSCs). Another resource related to physiology is available here.
Tanner Staging
Sex-specific physical characteristics can be evaluated with Tanner staging, which represents a predictable set of steps that males and females go through during puberty. It divides the development of secondary sexual characteristics into five stages. For females, breast (B1–B5) and pubic hair (Ph1–Ph5) development are staged (Table 3.1). For males, the genitals (G1–G5) and pubic hair (Ph1–Ph5) are staged (Table 3.2).
| Females (usually begins around 10–14 years old) | STAGE | BREAST | PUBIC HAIR |
|---|---|---|
| 1 | Prepubertal | Prepubertal |
| 2 | Slight enlargement of the papilla diameter (breast bud) | Sparse, long, slightly pigmented and curly hair along the labia |
| 3 | Further enlargement of the breast and areola with loss of contour separation between the breast and areola | Darker, coarser and curlier hair which progressively spreads over the mons |
| 4 | Areola and papilla form a secondary mound above the breast | Hair has increased in amount but is still limited to the mons |
| 5 | Mature areola and projection of only the papilla | Hair is distributed as an inverse triangle and spreads to the medial surface of the thighs |
| Note: Breast development may be unilateral for several months. | ||
| Males (usually begins around 12-16 years old) | STAGE | GENITALS | PUBIC HAIR |
|---|---|---|
| 1 | Prepubertal | Prepubertal |
| 2 | Testes and scrotum enlarge and there is reddening and a change in texture of the scrotal skin | Sparse growth of slightly curly and pigmented hair at the base of the penis |
| 3 | Continued growth of scrotum and testis. Penis grows (mainly in length) | Hair is darker, coarser and curlier and spreads of junction of the pubes |
| 4 | Further growth of penis, testes and scrotum with the development of the glans and darkening of the scrotum | Hair covers the pubes |
| 5 | Adult stage | Hair spreads over the medial surface of the thighs |
Age of Onset of Puberty
The normal age of onset of puberty and the development of SSCs depends on:
- Genetics
- Overall health
- Body fat and/or body composition
- Social environment
| Age at Development of SSCs in Boys | Age at Development of SSCs in Girls |
|---|---|
|
|
|
DISORDERS OF PUBERTY
Delayed Puberty
Definition
It is the absence or incomplete development of SSCs by an age 2–3 standard deviations above the mean age of onset of puberty (14 years for boys and 13 years for girls/no menarche by 15 years for girls).
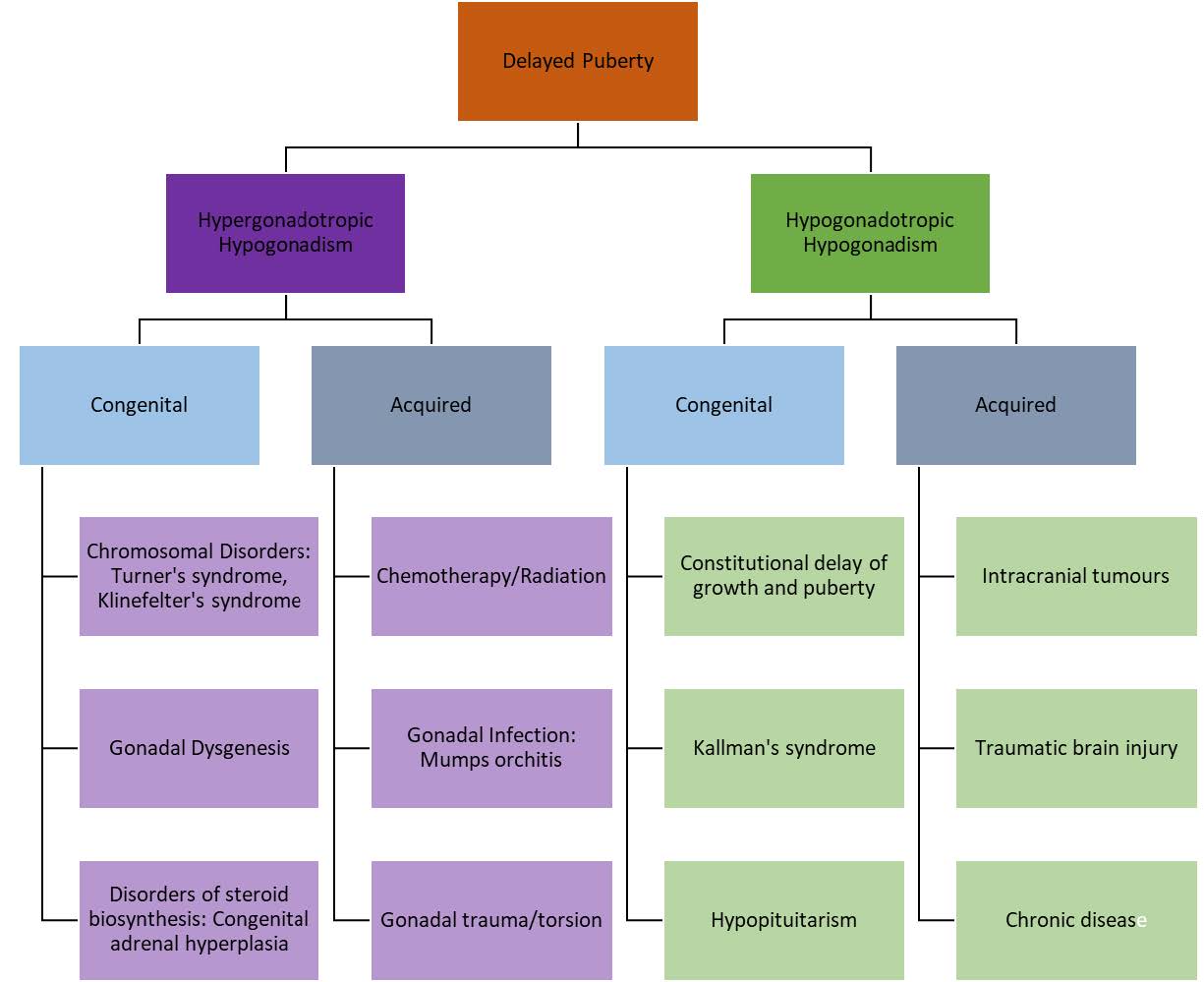
Aetiology and Classification
Delayed puberty may be due to hyper- or hypogonadotropic hypogonadism.
| HYPERGONADOTROPIC (PRIMARY) HYPOGONADISM | HYPOGONADOTROPIC (SECONDARY) HYPOGONADISM |
|---|---|
| There is failure of sex hormone (oestrogen and testosterone) production by the gonads i.e. there is ‐‐ FSH and LH, – oestrogen/testosterone | There is hypothalamic or pituitary dysfunction, resulting in FSH and LH levels and, thus, low sex hormones levels i.e. there is – FSH and LH, – oestrogen/ testosterone |
Diagnosis
It is made based on:
- History – a detailed history should be taken (screen for the many possible physical and functional causes of delayed puberty)
- Observation and examination – measure height, weight and head circumference, thoroughly examine all systems, perform Tanner staging and review previous growth records
- Investigations – perform blood tests (LH, FSH, oestrogen/testosterone, TSH, prolactin routine bloods, karyotyping), get imaging (bone age X-ray, pelvic US, abdominal US, brain MRI) and other special investigations (GnRH test, hCG stimulation test)
Management
One must identify and treat the underlying pathological cause of precocious puberty. A GnRH analogue may need to be given. Psychological support is essential.
Precocious (Early) Puberty
Definition
It is the onset of SSCs at an age 2–3 standard deviations below the mean age of onset of puberty (9 years for boys and 8 years for girls/menarche before 9 years for girls).
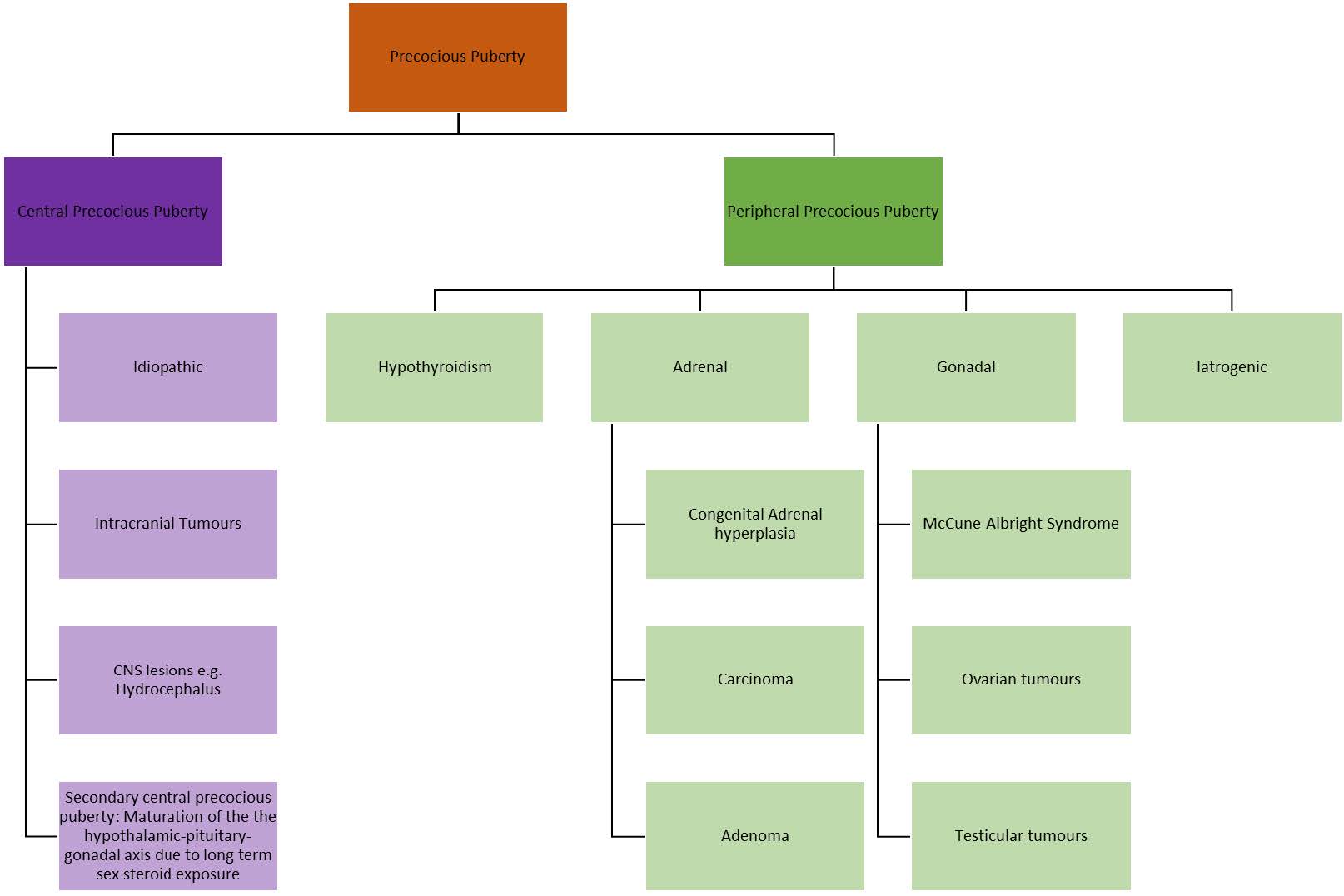
Aetiology and Classification
Precocious puberty can either have a central or peripheral origin.
| CENTRAL (GONADOTROPIN-DEPENDENT) PRECOCIOUS PUBERTY | PERIPHERAL (GONADOTROPIN-INDEPENDENT) PRECOCIOUS PUBERTY |
|---|---|
| Puberty occurs as a consequence of early physiological (true) activation of the hypothalamic-pituitary-gonadal (HPG) axis i.e. ↑FSH and LH, ↑oestrogen/testosterone | Puberty is due to a mechanism that does not involve the physiological HPG axis. The resultant elevated sex hormones levels trigger the development of SSCs. The sex hormones may be endogenous (gonadal or extragonadal) or exogenous. The endogenous sex hormones are made independently of the HPG – there is no secretion of FSH/LH to trigger the testes or ovaries to produce sex hormones i.e. – FSH and LH, oestrogen/testosterone |
Diagnosis
A diagnosis is made based on the demonstration of progressive pubertal development and increased growth rate, and laboratory evidence of increased sex hormone production.
A detailed history should be taken, with a focus on:
- Age when first signs of pubertal developmental observed
- Which features of puberty are present and in what order did they appear
- Evidence of growth acceleration
- Family history
- Systemic enquiry
The physical examination should include measurement of the height, weight, head circumference, a thorough systemic examination and assessment of SSCs for Tanner staging. One must also review the child’s previous growth records.
Investigations should include:
- Blood tests – LH, FSH, oestrogen/testosterone, TSH, serum androgen levels (17 OH-progesterone, DHEAS, androstenedione)
- Radiological tests – bone age X-ray, pelvic US, abdominal US, brain MRI
- Other special investigations – GnRH test
Management
It includes treating the underlying cause, sex hormone therapy and the provision of psychological support.
APPROACH TO GROWTH DISORDERS
Growth is a dynamic process (involves changes over time) that is a sensitive barometer of health. Growth monitoring is important for assessing the general health of the child (normal growth is an indicator of good health). When poor growth is detected, one should look for a treatable cause. Malnutrition and systemic illness are associated with growth abnormalities. When evaluating abnormal growth, one needs to exclude nutritional deficiencies and systemic illness.
Phases and Parameters of Growth
The following parameters are measured when assessing the growth of children – length/height, weight, head circumference and mid-upper arm circumference (MUAC). When assessing growth over time, one must determine:
- If the growth is steady, slowing or accelerating
- What sort of growth should be happening in this child at this time
Children experience growth in three phases:
- Infantile growth – from conception and into the first year of life; this growth phase is almost entirely dependent on nutrition
- Childhood growth – is influenced by genetics, nutrition and growth hormone (GH) levels
- Pubertal growth – is influenced by both GH and sex hormone levels
Endocrine Causes of Abnormal Growth
They may be grouped according to the child’s presentation or the pattern of growth:
- Short and fat – hypothyroidism, Cushing’s syndrome
- Slow growth in length/height – GH deficiency, sex hormone deficiency, hypothyroidism
- Fast growth in length/height – excess GH, excess sex hormone, hyperthyroidism
THYROID DISORDERS
Normal Physiology
The hypothalamus produces thyrotropin-releasing hormone (TRH) which stimulates thyroid stimulating hormone (TSH) production and secretion in the pituitary gland. TSH, in turn, stimulates the production and secretion of thyroxine (T4) and triiodothyronine (T3) by the thyroid gland (see related image here). T4 can be converted to the active form, T3. T4 is predominantly bound to T4-binding globulin. Serum T4 regulates the secretion of both TRH and TSH by means of negative feedback loops. The synthesis of thyroid hormone requires the presence of iodine.
Thyroid hormones affect every cell in the body, as they:
- Regulate the rate at which calories are burned (affecting weight loss or weight gain)
- Can slow down or speed up the heartbeat
- Can raise or lower body temperature
- Influence the rate at which food moves through the GIT
- Control the way muscles contract
- Control the rate at which dying cells are replaced
Hypothyroidism
Definition
It is a condition in which there is a thyroid hormone deficiency.
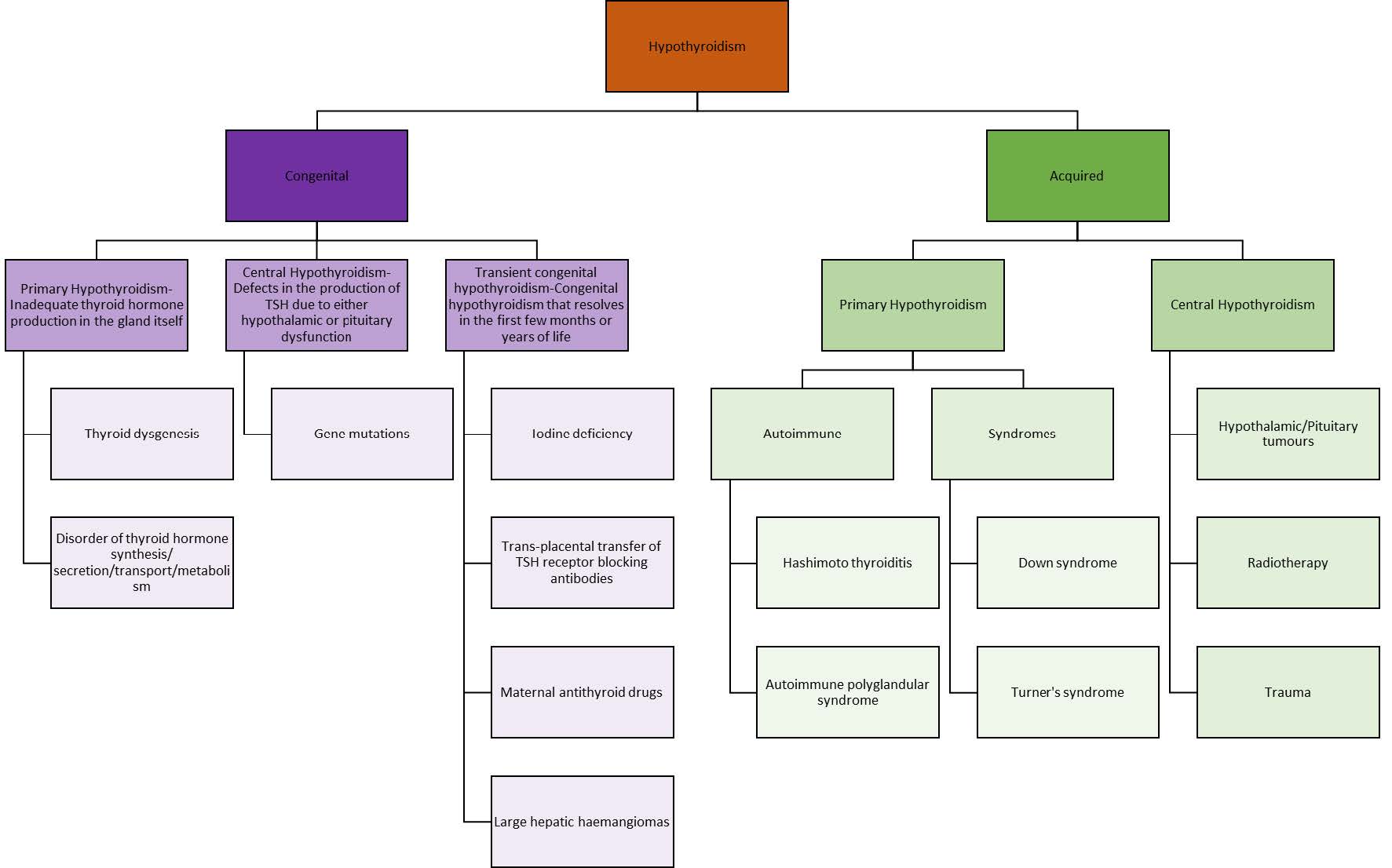
Aetiology and Classification
Hypothyroidism may be congenital or acquired (fig.3.3)
Clinical Features
| CONGENITAL HYPOTHYROIDISM | ACQUIRED HYPOTHYROIDISM |
|---|---|
|
Clinical features are non-specific and difficult to detect in the first month of life. They include:
|
They include:
|
Complications
If left untreated, the following complications may occur:
- Neurodevelopmental delay
- Poor motor coordination
- Hypotonia
- Ataxia
- Poor growth and short stature
Investigations
They should include:
- Serum TSH concentration (primary [normal/high] vs secondary hypothyroidism [low])
- T4 (free and total) and T3 (free or total)
- Serum antithyroid antibody test
- Thyroid ultrasound
- Radionucleotide scanning
Management
One must find the underlying cause and appropriately manage. Oral thyroid hormone replacement (levothyroxine) may be required. The patient should be followed up and thyroid hormone levels monitored.
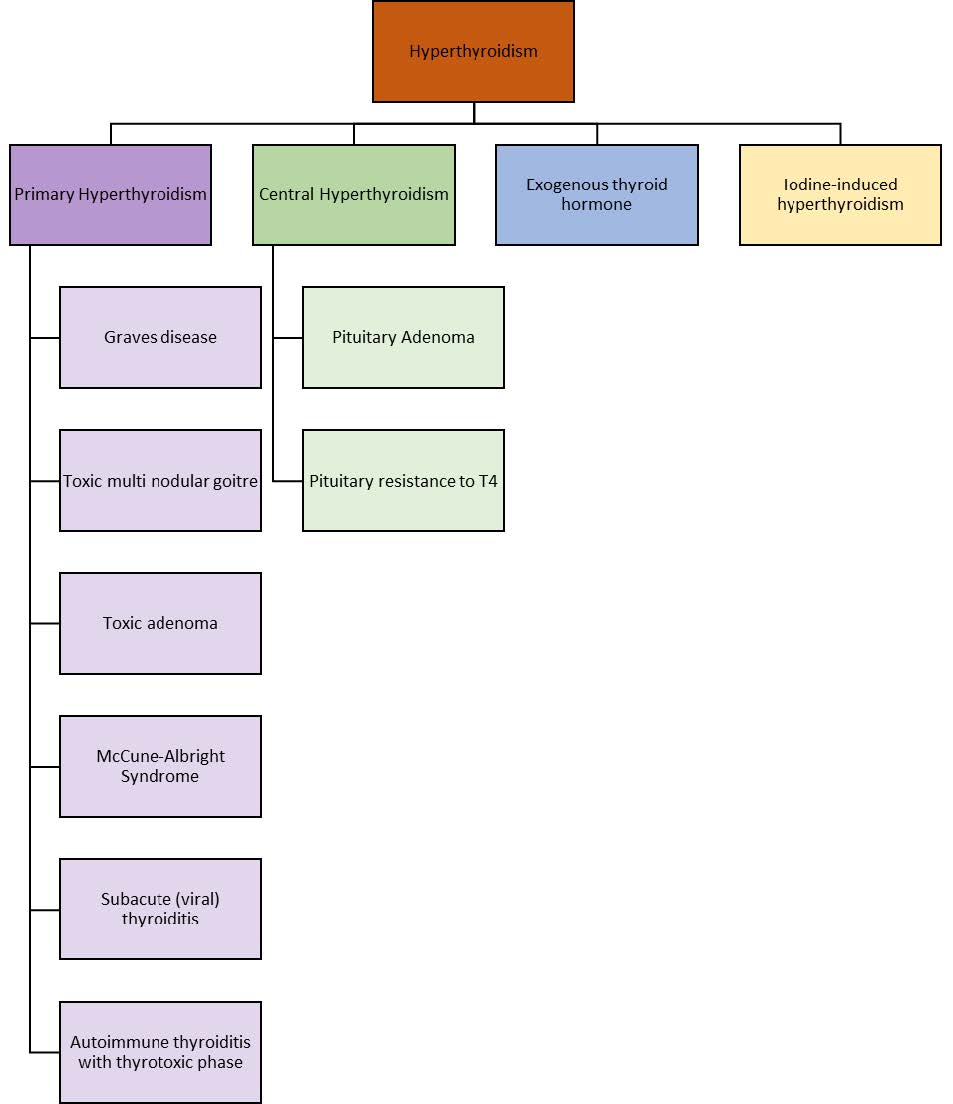
Hyperthyroidism
Definition
It is characterised by hyperfunction of the thyroid gland, leading to a state of thyrotoxicosis (clinical, physiological and biochemical findings that are the result of tissue exposure to excess thyroid hormone).
Aetiology
The most common cause of hyperthyroidism is Graves disease.
Clinical Features
- Hyperactivity
- Irritability
- Poor concentration
- Insomnia
- Heat intolerance
- Fatigue
- Muscle weakness
- Altered bowel habits
- Menstrual irregularity
- Tachycardia
- Hyperreflexia
- Fine tremor
- Weight loss despite increased appetite
Investigations
They should include:
- Serum TSH concentration
- T4 (free and total) and T3 (free or total)
- Serum antithyroid antibody test
- Thyroid ultrasound
- Radionucleotide scanning
Management
One must find and treat the underlying cause. One should give antithyroid drugs (e.g. carbimazole, propylthiouracil) and manage thyrotoxic symptoms (a 𝛽𝛽-bocker may be given to manage the anxiety, tremor and tachycardia). The patient should be followed up to monitor thyroid levels.
DIABETES MELLITUS (DM)
Definition
DM is a condition in which the body is unable to process glucose due to an insulin insufficiency. There are various types of DM, including:
- Type 1 DM (most common type in children)
- Type 2 DM
- Gestational diabetes
Pathophysiology
Type 1 DM is the result of autoimmune destruction of the insulin-producing 𝛽𝛽-cells in the islets of Langerhans in the pancreas (see related image here). This process occurs in genetically susceptible people and is triggered by one or more environmental agents. It usually progresses over many months or years, during which the individual is asymptomatic and euglycaemic.
Clinical Features
The child may present with:
- Polyuria
- Polydipsia
- Nocturia/nocturnal enuresis
- Weight loss
- Fatigue
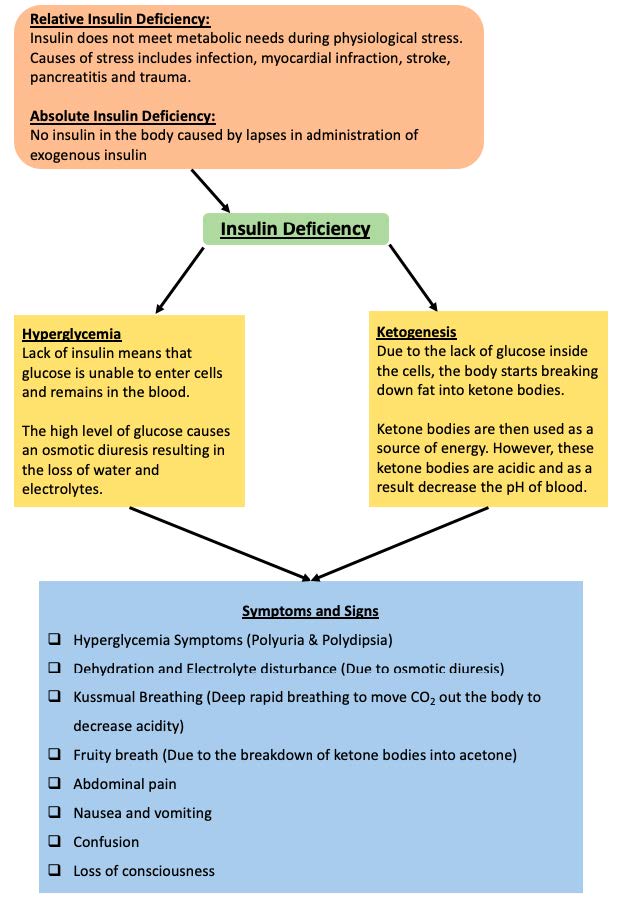
- Ketoacidosis (vomiting, deep sighing respiration, decreased level of consciousness and abdominal pain)
Investigations
The following investigations should be performed:
- Arterial blood gas
- Random blood glucose (will be >11.1 mmol/L in the diabetic patient)
- Fasting plasma glucose (will be >7 mmol/L on more than one occasion in the diabetic patient)
- Glycated haemoglobin (HbA1c)
- RFTs and electrolytes
- Diabetes-related autoantibodies e.g. islet cell antibody (ICA), anti-insulin antibody (IAA), anti-glutamic acid decarboxylase (anti-GAD) antibody
- Screening tests for other autoimmune diseases e.g. thyroid function tests/thyroid antibodies, coeliac antibody screen
Complications
They include:
- Diabetic ketoacidosis
- Microvascular complications – diabetic retinopathy, peripheral neuropathy, diabetic nephropathy
- Macrovascular complications – cerebrovascular accident, coronary artery disease, peripheral vascular disease
Management
It will include:
- Insulin therapy
- Education of the child and family about DM
- Nutritional management
- Monitoring of glycaemic control
- Avoidance and management of hypoglycaemia
- Management of acute illness and avoidance of DKA
- Screening, prevention and treatment of the micro- and macrovascular complications of DM
HYPOGLYCAEMIA
Definition
Hypoglycaemia is defined as a plasma glucose level that is low enough to cause signs and symptoms of brain dysfunction (neuroglycopenic symptoms). Glucose below 2.8 mmol/L is considered to be low.
Aetiology
Hypoglycaemia may be caused by:
- Acute or critical illness e.g. sepsis, liver failure, diarrhoea in the setting of malnutrition
- Drugs e.g. oral hypoglycaemic agents, salicylates, 𝛽𝛽-blockers
- Insulin mediated disorders e.g. hyperinsulinism, insulinoma
- Disorders of glycogen metabolism
- Disorders of gluconeogenesis e.g. glycogen storage disease type 1, fructose-1,6-bisphosphatase deficiency, galactosemia
- Hormone deficiencies e.g. cortisol deficiencies, growth hormone deficiencies, pituitary hormone deficiencies
- Hormone deficiencies e.g. cortisol deficiencies, growth hormone deficiencies, pituitary hormone deficiencies
Clinical Features
The child may present with:
- Autonomic symptoms:
- These are early symptoms and include sweating, tachycardia, weakness, tremor, and anxiety or feeling of nervousness, and/or severe hunger
- Neuroglycopenic symptoms:
- These symptoms develop with prolonged or severe hypoglycaemia
- They include lethargy, irritability, confusion, uncharacteristic behaviour, and hypothermia
- In extreme cases, there may be loss of consciousness, seizure, or coma
Infants may present with non-specific symptoms of irritability, feeding problems, lethargy, cyanosis, tachypnoea, and hypothermia.
Investigations
One should perform:
- Fingerpick and serum glucose
- LFTs
- Electrolytes
- Serum insulin, lactate, ketones, growth hormone, cortisol, C-peptide, amino acids and carnitine profile
- Urinalysis (look for ketones and glucose-reducing substances)
- Toxin screen
Management
Immediate management includes the administration of glucose/dextrose (orally in a conscious patient and IV in a patient with an altered level of consciousness or who is too young to drink it) and regular glucose monitoring. The dextrose infusion should be accordingly adjusted. One must then find and treat the underlying cause.