Chapter 10:CHILD AND ADOLESCENT PSYCHIATRY
Student Author: Asiphile Moyake
Specialist Advisors: Dr Papani Gasela and Dr Kaveshin Naido
This chapter covers the following topics:
- Attention deficit hyperactivity disorder (ADHD)/hyperkinetic disorder
- Anxiety disorders
- Suicide risk assessment
- Autism spectrum disorder (ASD)
- Enuresis
- Encopresis
- Other psychiatric disorders
ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD)/HYPERKINETIC DISORDER
Definition
It is defined as persistent inattentiveness, hyperactivity, impulsivity, disinhibition, and/or distractibility. These symptoms may all be transitory and part of normative developmental patterns (see ADHD related word cloud here). However, ADHD can be diagnosed if the symptoms impair daily living.
It is important to be able to recognise and manage ADHD because it is common, can be serious, can be persistent, is often stigmatised and is treatable.
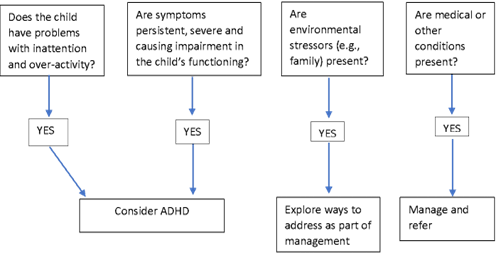
Diagnosis
The diagnosis is exclusively made on clinical grounds. The child must have:
- 6 of 9 inattentive symptoms and/or 6 of 9 hyperactive-impulsive symptoms
- Symptoms for at least 6 months
- Symptoms starting before age 12
- Symptoms in ≥2 or more situations e.g. home, school, extracurricular activities
- Significant difficulty with school, social or activities of daily living as a result of the symptoms
The symptoms must also not be attributable to another cause e.g. medical condition, intoxication, emotional distress.
Table 10.1: Differential Diagnoses for ADHD
|
Differential Diagnoses These psychiatric conditions can mimic ADHD:
|
Classification and Clinical Features
ADHD is classified as one of the following subtypes:
- Predominantly hyperactive/impulsive symptoms
- Predominantly inattentive symptoms
- Combined inattentive and hyperactive/impulsive symptoms
Table 10.2: Clinical Features of Inattentive- and Hyperactive-Type ADHD
| INATTENTIVE SYMPTOMS | HYPERACTIVITY-IMPULSIVE SYMPTOMS |
|---|---|
|
|
These symptoms may manifest differently depending on the child’s age:
- Preschool age – plays for <3 mins, does not listen, has no sense of danger
- Primary school age – performs activities for <10 mins, is forgetful, distracted, restless, intrusive and/or disruptive
- Adolescence – can attend for <30 mins, has difficulty focusing and/or planning, is fidgety and reckless
Associated features include:
- Defiance, aggression and antisocial behaviour
- Problems with social relationships
- IQ lower than the general population
- Specific learning problems
- Coordination problems
- Specific developmental delay
- Poor emotional self-regulation
The consequences of all this are that the child may have poor performance in school or sport, may become withdrawn, anxious or socially isolated and may be prone to accidents.
Clinical Assessment
It should consist of the following:
- Interviews with the child, caregivers and teachers
- One must get information about the child in at least two contexts/settings.
- One must also get a family history (ask parents if they had similar difficulties themselves or with their other children).
- Medical and psychiatric assessment (also assess for psychiatric comorbidities)
No additional tests are necessary to make the diagnosis, as it is made on clinical grounds according to the DSM-5 and ICD-10. However, rating scales are used as screening tools and are useful for monitoring symptoms at baseline and once treatment has been initiated. An example of this is the Swanson, Nolan and Pelham Rating Scale (SNAP IV), which is completed by both teachers and parents.
Psychiatric Assessment (Mental State Examination)
One must observe the relationship between the child and parent(s) in the consulting room. Often, due to difficulties related to ADHD, the parent-child relationship may be very strained.
During the consultation, the child may have difficulty sitting still and may make inappropriate interruptions. S/he may climb over furniture or leave the consultation early. One must observe how the parent performs limit-setting and enforces boundaries during the consultation.
For children on methylphenidate or other medication, it is important to ask whether the child has taken his/her medication that day and at what time it was taken. This may influence the clinical picture and whether ‘top-up’ doses of medication are needed.
Medical Assessment
One must exclude any comorbidities or other medical conditions that could better explain the patient’s symptoms.
One must measure and plot growth parameters e.g. height-for-age, weight-for-age. Blood pressure measurement, pulse monitoring and cardiac examination are also important, especially if the child is on stimulants.
If there is a family history of sudden cardiac death, one must do an ECG and consult with a paediatrician.
Management
The aims of treatment in the child with ADHD are to reduce symptoms, improve educational outcomes and reduce family and school-based problems.
Non-Pharmacological Management
It includes school and home-based behavioural interventions. The parents and teachers should, therefore, receive psychoeducation and the child should be referred to a mental health service, as behavioural interventions are effective in mild-to-moderate cases.
Parents should receive management training and support. They must be taught to constructively deal with their child’s behaviour, by teaching them how to positively reinforce desirable behaviours and extinguish misbehavior. This is a first-line intervention for younger children and mild cases of ADHD.
One must also liaise with the school and, if appropriate, ask for extra help for the student e.g. sit the child in the front of class, give short tasks, give extra time to complete assessments.
Pharmacological
One may prescribe:
- Stimulant medications:
- They have the best evidence of effectiveness in the management of the child with ADHD.
- Short-acting oral methylphenidate may be prescribed by a general practitioner at a maximum dose of 1 mg/kg/day. Its effects last 3-4 hours.
- Long-acting oral methylphenidate-long may be prescribed alone or with short-acting methylphenidate (if giving combined treatment, make sure that both doses do not exceed 1 mg/kg/day). Its effects last 6-8 hours.
- Extended-release methylphenidate (e.g. Concerta® lasts ~12 hours and must be prescribed by a psychiatrist or paediatrician.
- Common side effects of these drugs are nausea, weight loss, insomnia, and agitation. More serious side effects are tics, psychosis, elevated blood pressure and growth retardation.
- Non-stimulant medications:
- They are less effective and may have adverse effects. Thus, they should only be prescribed when stimulants are not appropriate or not tolerated.
- Atomoxetine is a selective norepinephrine reuptake inhibitor (SNRI) which is used as a second-line agent when there are serious side effects to methylphenidate (see related image here), comorbidities, risk of drug diversion and to treat comorbid anxiety. It must be prescribed by a psychiatrist.
- Clonidine is an α1‐ agonist and is a third-line agent which is specialist-initiated.
Referral
One should refer the child who:
- Is <7 years old and in whom one suspects ADHD
- Has shown no response to treatment after 8 weeks
- Has intolerable side effects to medication
- Has an uncertain diagnosis
- Has comorbid psychiatric conditions, including substance use
- Has uncontrollable seizures
- Is post TBI
- Is RVD positive
Prognosis
Up to 60% of ADHD cases will continue into adulthood, however the symptoms may vary with time.
ANXIETY DISORDERS
Children may suffer from anxiety disorders, such as separation anxiety disorder, specific phobia, generalised anxiety disorder, social anxiety disorder and panic disorder. Post-traumatic stress disorder and obsessive-compulsive disorder may also be diagnosed during childhood and adolescence. However, the DSM-5 no longer classifies these under anxiety disorders.
Definition
Fear is a reaction to a real threat, whereas anxiety is the cognitive, emotional and physiological reaction to a real or imagined threat. Both anxiety and fear can be adaptive. Many childhood anxieties are developmentally appropriate, thus it is important to keep the age and developmental stage of the child in mind. An anxiety disorder may be diagnosed when the anxious reaction results in psychic distress and/or interferes with daily functioning. The fears and anxiety are usually out of keeping with the child’s developmental stage.
Anxiety disorders are the most common psychiatric disorders in childhood and are associated with a poor quality of life, depression and social limitations. Often, children with panic disorders are labelled with treatment-resistant asthma.
Anxiety disorders are often comorbid with other anxiety disorders, depression or behavioural disorders, see related image here.
Classification and Clinical Features:
The child with anxiety will develop maladaptations, which are
- Behavioural e.g. avoidance of situations that may result in the feared event
- Cognitive e.g. distress over a feared event that may occur
- Physiological e.g. autonomic symptoms of sympathetic nervous system
Clinical features specific to the anxiety disorder are shown in the table.
Table 10.3: Clinical Features of Various Anxiety Disorders
| Anxiety Disorder | Clinical Features |
|---|---|
| Separation anxiety disorder |
|
| Selective mutism |
|
| Specific phobia |
|
| Social anxiety disorder |
|
| Panic disorder |
|
| Agoraphobia |
|
| Generalised anxiety disorder |
|
Aetiology
Anxiety disorders may develop because of:
- Witnessing abuse or violence
- Neglect
- Frequent relocation
- Serious illness in the child or caregiver
- School-related issues e.g. bullying, poor academic performance
- Death of a close relative
- Learnt fears
- Difficulties with primary attachment
One must get a detailed history from the child and parents as the anxiety may be warranted for the child’s context e.g. abuse.
Management
Non-Pharmacological Management
This may include:
- Psychotherapy – it is important to psychoeducate the child and parents about anxiety and the appropriate management thereof; may be individual or group therapy
- Cognitive behavioural therapy (CBT)
- Skills-based programs – usually consist of psychoeducation, relaxation techniques, exposure, contingency management, cognitive restructuring, social skills, assertiveness training and parent training
Pharmacological Management
Medication is used in severe cases. One may prescribe:
- Benzodiazepines – short term; use with extreme caution in children and for no longer than 2 weeks as it can lead to paradoxical disinhibition and can potentially lead to dependence and avoidance of anxiety
- Antidepressants – long term; selective serotonin reuptake inhibitors (SSRIs) are generally used for anxiety (fluoxetine is the only SSRI licenced for use in children)
Referral
The child should be referred to a child and adolescent psychiatry service if s/he has a poor response to treatment, s/he has psychiatric co-morbidities, there is a need for diagnostic clarification or there is no access to psychotherapeutic services at primary or secondary healthcare levels.
Prognosis
These children are at higher risk for anxiety disorders, mood disorders, suicidality and substance use disorders in adulthood.
SUICIDE RISK ASSESSMENT
Suicidality in children may be underestimated as it may be misinterpreted as the child or adolescent is ‘seeking attention’ or ‘acting out’. Unless otherwise specified, suicidality is a broad term that refers to the cognitions, activities or behaviour of persons seeking their own death, including thoughts/ideations, utterances, threats, plans, intent, actions or omissions.
Whereas, suicidal behaviour refers to any behaviour that is often intentional, potentially harmful or lethal to the child. It is the result of psychological pathology or a reaction to adverse life events. Suicidal behaviour may also be a reaction to abuse (physical, emotional or sexual), neglect or poor home circumstances. This needs to be explored in detail in a child or adolescent who presents with suicidality.
Criteria and Clinical Features
The criteria for suicidality include:
- Suicide attempt within last 24 months
- Not attempted suicide in a state of cognitive impairment e.g. delirium, confusional state
- Does not meet non-suicidal self-injury criteria
- Not applied to suicidal ideation
The child may present with a history of:
- Well planned, lethal attempt
- Failed suicide attempt
- Unplanned, impulsive acts
- Threats of suicide
Associated Comorbidity
The child may have a psychiatric disorder at the time of the suicide attempt. Common comorbid conditions include:
- Conduct disorders
- Major depressive disorder
- Eating disorder
- ADHD
- Personality disorders:
- Although one cannot diagnose a personality disorder in someone <18 years, an adolescent can present with emerging traits of certain personality disorders e.g. borderline personality disorder.
- Traumatic stress disorders e.g. PTSD
The child may also have:
- Poor relationship with caregiver or parent
- Poor emotional support
- Experienced neglect
- Parent-child relational difficulties
- Experienced harsh, punitive or inconsistent discipline and boundary-setting by parents/caregivers
Management
Management should be individually tailored and should consider risk factors specific to individual patients. One must:
- Conduct a risk assessment – assess current severity and intensity of ideations and behaviour, lethality of plans and access to lethal means
- Take a detailed history of predisposing, precipitating, perpetuating and protective factors
- Identify comorbid depression, psychosis, substance abuse and conduct disorder
- Manage co-morbid conditions
The treatment plan should include psychotherapeutic, psychopharmacological and/ or social interventions to achieve relief from acute psychosocial stressors. However, the interventions employed will largely depend on the clinical services available.
Principles of Management
They include:
- Actively involving the patient and parent(s) in the planning and implementation of interventions
- Referral to child psychiatry
- Supporting the family through other issues e.g. divorce, parental mental illness substance misuse
- Organising support from social services and child welfare agencies, if indicated
- Organising relief from excessive demands e.g. school demands exceeding patients’ current capacity
- Treating underlying psychiatric disorders
- Regularly monitoring for recurrence of suicidal behaviour
- Developing a post-discharge emergency and safety plan for an acute suicidal crisis
- Offering flexible treatment sessions (adapt time and frequency to the patient’s needs)
- Developing strategies to improve adherence to treatment (short, accessible interventions)
- Effectively communicating with all the professionals involved (social worker, psychotherapist, child and adolescent psychiatrist, paediatrician or general practitioner)
See related image here.
Admission
Hospitalisation is generally indicated if:
- There is a high suicide risk, especially if there are no alternative ways of ensuring the patient’s safety
- The patient has had a recent suicide attempt requiring intensive medical care
- It is not possible to reliably estimate suicide risk
Ideally, inpatient treatment of a child should be in a secure child psychiatry ward or paediatric ward and ensure close supervision, monitoring and support of the patient.
Non-Pharmacological Management
The child should be offered psychotherapy – CBT and dialectical behavioural therapy (DBT). DBT adapted for use in adolescents with suicidal behaviour involves training in mindfulness, interpersonal skills, emotion regulation, and stress tolerance. The parents should be involved in the psychosocial interventions and strategies to improve the parent-child relationships implemented e.g. improving problem solving within the family, parenting techniques and communication skills. See related image here.
AUTISM SPECTRUM DISORDER (ASD)
See the Disorders of Development chapter.
ENURESIS
It is the voiding of urine into clothing or in bed after the age of 4-5 years i.e. intermittent urinary incontinence.
Classification
It may be clinically classified as:
- Monosymptomatic:
- The child has enuresis (diurnal or nocturnal) without daytime lower urinary tract symptoms.
- This type of enuresis is more common in children >5 years old.
- Non-monosymptomatic:
- The child has enuresis (diurnal or nocturnal) with daytime lower urinary tract symptoms e.g. urgency, incontinence, increased voiding frequency.
- In these children, one must exclude serious pathologies, such as ectopic ureteric insertion and tethered cord syndrome.
Nocturnal enuresis may be primary (the child has never gained bladder control; more common) or secondary (the child had gained bladder control for >6 months but now has recurrent bedwetting). Nocturnal enuresis should not be over-investigated.
Aetiology
Causes or precipitating events include:
- Medical conditions:
- UTI
- Diabetes
- Epilepsy
- Bladder instability
- Low bladder capacity
- Nocturnal polyuria (decreased vasopressin levels at night
- Lack of arousal from sleep
- Other neurological disorders
- Traumatic events in the child’s life
- Birth of a new sibling
- Family relocation
- Parental separation
- Disturbed behaviour
- Depressed mood
Assessment
Evaluation should include:
- Detailed history (noting any social or psychological problems)
- Thorough physical examination
- Morning urine dipsticks (paying special attention to specific gravity)
Management
It includes:
- Non-pharmacological interventions:
- Increasing daytime fluid intake
- Treating constipation
- Restricting fluid intake near bedtime and avoiding caffeinated beverages
- Voiding the bladder before bed
- Increasing bladder capacity
- Dry bed training
- Following a quiet bedtime routine
- Using a night light and bedding protection
- Waking the child to urinate during the night (night-time lifting)
- Employing alarm therapy and a pad system (very effective but takes a few weeks to work)
- Positive reinforcement – reward the child for dry nights and self-arousal e.g. a star chart and rewards (an activity that child and parent enjoys doing together) for maintaining dryness; not a monetary reward or screen time
- Refer the child for psychological evaluation
See related image here.
- Pharmacological interventions (may be tried in the child <7 years old):
- Imipramine (10-25 mg at bedtime; titrate up in older children) – there is a risk of cardiotoxicity
- Desmopressin:
- It may increase control when added to other drug therapies.
- It can be kept for special occasions when bedwetting is particularly undesirable e.g. sleepovers.
- It should not be taken with excessive amounts of water later in the day or in the early evening.
- Oxybutynin hydrochloride (give early in the evening/with supper)
- Tolterodine tartare (give early in the evening/with supper)
ENCOPRESIS
It is the (usually involuntary) voiding of faeces in inappropriate spaces (according to social or cultural norms) after the age of 4 years in a child who has obtained bowel control.
Aetiology
Causes include:
- Anxiety-related diarrhoea
- Psychological factors e.g. expressing anger, response to traumatic event
Assessment
A detailed history must be taken and medical/organic causes excluded e.g. Hirschsprung’s disease, spina bifida, cord lesions, overflow incontinence in the chronically constipated patient.
Diagnostic Criteria
They include:
- Repeated passage of faeces in inappropriate places (involuntary or intentional)
- At least one such event a month for at least 3 months
- Chronological age ≥4 years (or an equivalent developmental age)
- Physiological causes or medical conditions have been excluded
Management
If a medical cause for the incontinence is found, it should be managed e.g. disimpaction and routine laxative therapy (polyethylene glycol, enemas) for the child with constipation. Behavioural therapy is effective (such as star charts). Parents must be educated on how to appropriately manage difficulties. The home circumstances must be assessed and prior history of traumatic events (including sexual abuse) elicited if present. The child should be referred to a child psychiatry and adolescent service if the encopresis is persistent.
If a medical cause for the incontinence is found, it should be managed e.g. disimpaction and routine laxative therapy (polyethylene glycol, enemas) for the child with constipation. Behavioural therapy is effective (such as star charts). Parents must be educated on how to appropriately manage difficulties. The home circumstances must be assessed and prior history of traumatic events (including sexual abuse) elicited if present. The child should be referred to a child psychiatry and adolescent service if the encopresis is persistent.
OTHER PSYCHIATRIC DISORDERS TO RECOGNISE
Psychotic Disorders
Psychosis in children is very rare. It is most often due to a general medical condition that produces psychotic features e.g. epilepsy, head trauma, inborn errors of metabolism, delirium. Medical causes of psychosis and the effect of illicit substances and substance withdrawal need to be ruled out before psychosis is diagnosed.
Childhood-Onset Schizophrenia (COS)
It is the onset of schizophrenia before the age 13 years, whereas early-onset schizophrenia (EOS) refers to the onset of schizophrenia before 18 years of age. It tends to develop in children aged 5-12 years.
Diagnostic Criteria
The diagnostic criteria for COS are the same as for schizophrenia in adults:
- ≥2 characteristic symptoms:
- These characteristic symptoms are hallucinations, delusions, disorganised speech, disorganised or catatonic behaviour and/or negative symptoms.
- During the active phase, hallucinations, delusions, or disorganised speech must be present.
- Duration of at least 1 month (or shorter if successfully treated)
- Persistence of symptoms for at least 6 months
- Associated significant decline in functioning:
- In children and adolescents, a decline in function may include the failure to achieve age-appropriate levels of interpersonal or academic development.
Perceptual disturbances are common. Auditory hallucinations are most common, however visual hallucinations are more common in children than in adults. Negative symptoms (amotivation, flat or blunted affect, poverty of speech and paucity of thoughts) and cognitive symptoms (impaired attention, memory and executive functioning) are very common and are usually the first to manifest (before hallucinations). Changes in mood, anxiety and agitation are also common.
Premorbid dysfunction, which may coexist, includes social withdrawal and isolation, disruptive behaviour problems, academic difficulties, speech and language problems, and cognitive delays.
Management
Antipsychotic medication is the primary treatment for schizophrenia spectrum disorders in children and adolescents. Maintenance medication is required to improve functioning and prevent relapse. In young people with treatment-resistant schizophrenia spectrum disorders, a trial of clozapine should be considered. Psychotherapeutic interventions should be implemented in combination with pharmacological interventions.
On follow-up, one must:
- Ask about medication-related adverse effects
- Ask about family history of cardiac disease or diabetes
- Repeat the physical examination, including height, weight, body mass index and waist circumference
- Perform laboratory investigations – FBC, urea, electrolytes, LFTs, fasting glucose and lipids (if on risperidone or olanzapine), and prolactin levels (if on risperidone)
Conduct Disorder
Definition
Conduct disorder is the persistent violation or defiance of age-appropriate norms, rules of society or expectations by a child over a 12-month period.
Diagnosis
The child with conduct disorder will:
- Show aggression towards people or animals e.g. violent behaviour, cruelty to animals (see related image here)
- Destroy property e.g. fire-setting, vandalism (see related image here)
- Be deceitful or steal (see related image here)
- Seriously violate rules e.g. stay out at night despite parental prohibitions, be truant
The child, caregivers and collaterals must be interviewed to obtain medical and social information. The above behaviours are displayed in the absence of a mood or psychotic disorder. It is particularly important to exclude abuse, maltreatment and neglect.
Comorbidity
Children with conduct disorder may also have:
- Learning problems
- ADHD
- Substance abuse disorder
- Antisocial behaviour
Management
The mainstays of management are family and behaviour therapy as well as parenting skills training. The child should undergo educational assessment and be offered school and emotional support. Placement in a child and youth care centre should be considered a last resort
Tic Disorders
Definition
A tic is a sudden rapid, recurrent, non-rhythmic vocalisation or purposeless motor movement. The tics are absent during sleep and are exacerbated by stress.
Classification
The child may have:
- Motor tics (facial, upper limb or torso tics are common) e.g. abnormal blinking, facial twitching, rude gestures
- Vocal tics e.g. shouts, repetition of specific words or phrases, swearing
Tic disorders may be classified as:
- Provisional tic disorder – single or multiple motor or vocal tics for <1 year
- Persistent (chronic) motor or vocal Tic Disorder – single or multiple motor or vocal tics for > 1 year
- Tourette’s disorder – multiple motor tics AND one or more vocal tics for > 1 year; often associated with OCD or ADHD
Management
The child, family and teachers should receive psychoeducation and the former two provided with emotional support. The child should be referred to child and adolescent psychiatry services for habit reversal therapy and pharmacological intervention. The child may be started on a low-dose of a first-generation antipsychotic (e.g. haloperidol) or second-generation antipsychotic (e.g. risperidone).
Mood Disorders
Depression
Children with depression present slightly differently to adults with depression. The depression may be precipitated by bereavement or environmental stress (such as family break-up) and is often associated with anxiety disorders.
Clinical Features
The child may have:
- Depressed mood
- Irritability (may have angry outbursts)
- Sadness and misery
- Tearfulness
- Loss of energy
- Changes in feeding and sleep pattern (can manifest as FTT despite adequate food intake)
- Changes or deterioration in academic performance
- Anxiety and social withdrawal
- Self-blame and inappropriate feelings of guilt
Comorbidity
Common comorbid conditions include:
- Anxiety disorders
- OCD
- PTSD
- Conduct problems
- ADHD
- Learning difficulties
Management
One must perform a detailed assessment to exclude medical causes for this presentation e.g. vitamin B12 deficiency, hypothyroidism, sexually transmitted infections. Psychosocial stressors must be explored in detail with the child, caregivers and teachers and these stressors managed. A social worker referral should be performed, if necessary.
Family counselling should be performed, particularly psychoeducation surrounding the diagnosis. The child should be assessed for suicide risk and referred for psychotherapy, particularly CBT. Antidepressants may be started after excluding BMD and the child has been deemed a low suicidal risk
Mania and Bipolar Mood Disorder (BMD)
BMD can start in childhood but has higher prevalence rates in adolescence. They present with persistent and rapidly changing moods (depression and mania).
Clinical Features
The child may have:
- Elevated or irritable mood
- Grandiosity inconsistent with the child’s development stage
- Hypersexuality unrelated to sexual abuse
- Decreased need for sleep
- Increased loquacity
- Flight of ideas or racing thought
- Distractibility
- Increased goal-directed activity or psychomotor agitation
Psychiatric Comorbidity
Comorbid conditions include:
- ADHD
- Disruptive behavior disorders
- Anxiety disorders
- Substance use disorders (in adolescents)
BMD is associated with fractured family and peer relationships, poor academic performance, chronic mood symptoms or mixed presentations, psychosis, suicide attempts and hospitalisations.
Assessment
One must assess if there is a family history of cardiac disease, diabetes or thyroid disease. Medical causes and the potential role of substances (both illicit and prescribed) must be excluded. A thorough physical examination should be performed, including height, weight, BMI and waist circumference. One should perform the following investigations:
- Pregnancy test (in adolescent females)
- Urine drug screen
- FBC
- RFTs
- TSH & free T4
- Calcium, magnesium and phosphate
- LFTs
- Lithium levels (if on lithium)
- Fasting glucose and lipids (if on risperidone or olanzapine)
- Prolactin levels (if prescribed risperidone)
Management
The child and caregivers must be provided with psychoeducation and advised on the importance of sleep hygiene and routine. They should be referred to a child and adolescent psychiatry service for further management. With acute episodes, one may treat the patient with a mood stabiliser e.g. second-generation antipsychotic, lithium or anticonvulsant.